Jugular bulb oximetry (SjvO₂)
A retrograde IJ catheter samples blood draining the brain, giving global cerebral O₂ extraction by the Fick principle; the historical reference for cerebral O₂ balance.
1. Bedside vignettes: why this matters
Vignette A. Severe TBI, hyperventilation titration
A 14-year-old with severe TBI, ICP 26 mmHg refractory to first-tier measures, started on controlled hyperventilation. The team aims for PaCO₂ 30 mmHg. With a retrograde IJ catheter in place, the bedside SjvO₂ falls from 68% to 52% as PaCO₂ falls to 28. AjvDO₂ widens. This is hyperventilation-induced ischaemia: the vasoconstriction has dropped CBF below the threshold of demand. PaCO₂ is corrected back to 32; SjvO₂ recovers to 62%. ICP holds. The SjvO₂ gave you the metabolic crash guardrail.
Vignette B. Pediatric post-cardiac-arrest, "luxury" SjvO₂
A 7-year-old after a 25-minute submersion arrest, day 2 post-ROSC, normothermic. SjvO₂ is 88% on a stable MAP. NIRS rSO₂ is 92%. The team is reassured. The aEEG is markedly suppressed; the SSEP shows bilateral absent N20. High SjvO₂ in a comatose post-arrest brain is luxury perfusion, not safety: flow without demand because demand has collapsed. Combined with the electrophysiology, the prognosis is poor.
Vignette C. Catheter drift gives a misleading low
A 16-year-old severe TBI day 3 with a previously stable SjvO₂ of 65%. The morning sample reads 40%. The team reaches for fluids and a vasopressor before the senior fellow points out that the catheter tip is no longer at the bulb on the chest film: it has drifted distally into the brachiocephalic confluence and is sampling extracerebral blood mixed with chest-wall venous return. The catheter is repositioned and the SjvO₂ returns to 64%. Position drift is the single most common SjvO₂ artefact; the daily chest film check matters.
2. What SjvO₂ is, and what it is not
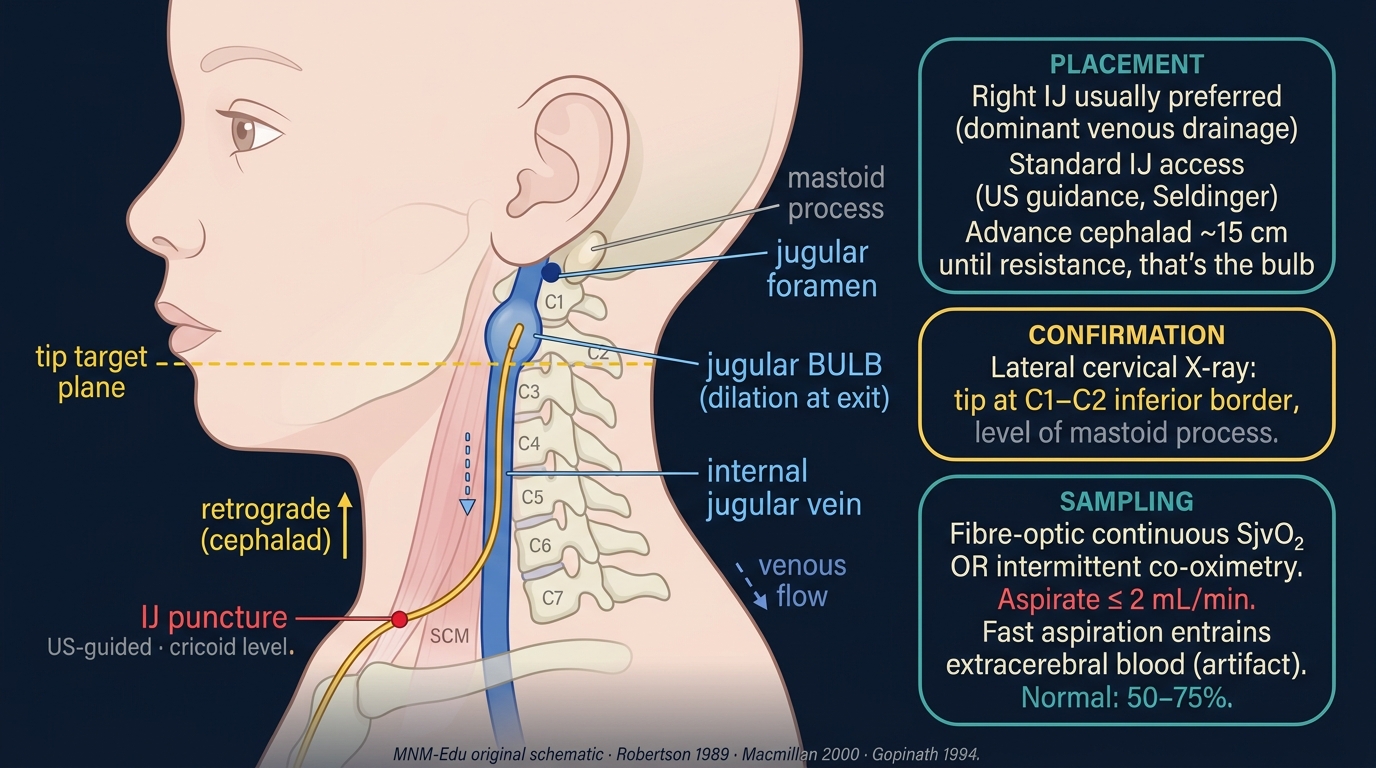
The jugular venous bulb is the dilation of the internal jugular vein at the base of the skull, where almost all blood draining the brain converges before mixing with extracerebral venous return downstream. A catheter advanced retrograde from the IJ up to the bulb samples blood that is, to first approximation, the global cerebral venous effluent.
The Fick principle ties SjvO₂ to cerebral O₂ balance:
Rearranging gives the O₂ extraction fraction:
Normal OEF is about 0.30 (35% extraction). When CBF falls relative to CMRO₂, OEF rises and SjvO₂ falls. When CBF is in excess of CMRO₂ (luxury perfusion, severe injury with collapsed metabolism), OEF falls and SjvO₂ rises.
| SjvO₂ band | Interpretation | Bedside meaning |
|---|---|---|
| > 85% | Luxury perfusion or low CMRO₂ | Hyperaemia, dead brain, deep sedation, hypothermia, AV shunting |
| 75–85% | Mild luxury | Sedation effect, hyperaemic phase of injury |
| 55–75% | Normal range | O₂ supply matches demand |
| 50–55% | Increased extraction | Low CBF, low CaO₂, or high CMRO₂; early concern |
| < 50% | Critical ischaemia | Imminent or established cerebral hypoxia |
| < 40% | Severe ischaemia | High risk of infarction; act now |
What SjvO₂ does well
- Global cerebral O₂ balance: a single number that captures the whole-brain supply-demand ratio.
- Hyperventilation titration: the canonical use; identifies the PaCO₂ at which vasoconstriction crosses into ischaemia.
- CPP / autoregulation cross-check: a low SjvO₂ with low CPP points to inadequate perfusion; a low SjvO₂ with adequate CPP points to a metabolic mismatch (fever, seizure, intra-cerebral shunting).
- Long-term ICU bedside trend: intermittent samples (every 4–8 h) plus continuous fibreoptic devices for high-resolution work.
What SjvO₂ cannot do
- Detect regional ischaemia: a regional infarct in 20% of cortex with the other 80% healthy will not move global SjvO₂ enough to alarm.
- See the watershed: the bulb mixes blood from the whole hemisphere; small territory ischaemia is invisible.
- Be interpreted without a chest film: catheter position drift is common and produces false readings.
- Replace PbtO₂: tissue-level oxygen tension at the most-at-risk parenchymal site is more sensitive to regional ischaemia and more actionable in modern protocols.
SjvO₂ is the whole-brain average. It is excellent for detecting global ischaemia (hyperventilation-induced, low-CBF states) and luxury perfusion, blind to focal ischaemia, and dependent on accurate catheter placement at the bulb.
Pediatric SjvO₂ is technically harder than adult: smaller jugular calibre, smaller bulb, more catheter-tip drift, and an IJ that follows the carotid more closely. Most modern pediatric ICUs use PbtO₂ instead when an invasive O₂ monitor is indicated. SjvO₂ remains the teaching reference and a fallback when PbtO₂ probes are unavailable or in centres without a parenchymal-monitoring programme.
3. Anatomy: the jugular bulb and its catheter
3.1 The bulb
The jugular bulb is the most rostral portion of the IJ; it dilates as the sigmoid sinus opens into it. Anatomic considerations:
- Right vs left dominance: most patients have a right-dominant venous drainage (60–70% of cerebral outflow). Conventional practice is to catheterise the dominant side.
- Determining dominance: compress each IJ in turn at the bedside; the side whose compression raises ICP more (or where ipsilateral compression produces a larger ICP rise) is dominant. In planned cases, MR / CT venogram or simple sonographic measurement of bulb diameter informs the choice.
- Bulb position: just below the jugular foramen, lying against the C1 transverse process; on a lateral skull film, the bulb sits between C1 and the lower border of the mastoid.
- Mixing with extracerebral venous return: blood from the face, scalp, and neck drains into the IJ below the bulb; a catheter tip that has slipped below the bulb samples mixed venous blood and over-reads (or under-reads) SjvO₂.
3.2 The catheter
Two types:
- Intermittent sampling catheter: a short multi-lumen central catheter advanced retrograde from the IJ to the bulb. Blood samples are drawn for co-oximetry every 4–6 hours.
- Continuous fibreoptic catheter (Oximetrix, Edwards SwanGanz-equivalent): a fibreoptic at the catheter tip continuously reads the spectral O₂ saturation; calibrated against intermittent co-oximetry every 12–24 h to correct for drift.
3.3 The chest film: not optional
Every SjvO₂ catheter gets a post-placement chest film (lateral skull if available) and a daily chest film thereafter. Position drift in either direction (too distal: samples mixed; too proximal: against the bulb wall, sluggish flow) is the single most common artefact.
An SjvO₂ value out of context is a number without a meaning. Always pair the value with: catheter position on the latest film, the sampling rate (was the sample drawn slowly?), the patient's CaO₂ (Hb, SaO₂), and the clinical state (sedation, temperature, ICP). Without these, the number is noise.
4. The signal: from sample to interpretation
Each SjvO₂ measurement gives a percent saturation; the bedside interpretation comes from comparing it with the arterial saturation to compute AjvDO₂ or OEF, and from setting the value against the CMRO₂ context (fever? seizure? sedation? hypothermia?).
4.1 The AjvDO₂ pair
In a healthy adult with Hb 12, SaO₂ 99%, SjvO₂ 65%: AjvDO₂ ≈ 5.5 mL/dL.
- AjvDO₂ < 4 mL/dL: low extraction; luxury perfusion or low CMRO₂.
- AjvDO₂ 4–7 mL/dL: normal range.
- AjvDO₂ > 7 mL/dL: increased extraction; the brain is working harder per unit blood; check CBF, CaO₂, CMRO₂.
4.2 The CEO₂ shorthand
A normal CEO₂ is around 0.30 (30% extraction). CEO₂ > 0.40 is concerning; CEO₂ > 0.50 is critical.
4.3 Slow sampling matters
The pulsatile / continuous nature of flow at the bulb means that fast aspiration of a sample contaminates the sample with extracerebral venous return retrogradely sucked up the IJ. Slow draw (over 30–60 seconds) yields clean cerebral venous blood.
5. The numbers to record: the SjvO₂ six-pack
| Variable | Symbol | What it tells you |
|---|---|---|
| Jugular venous saturation | SjvO₂ | Primary metric; 55–75% normal |
| Arterial saturation | SaO₂ | Required for AjvDO₂ and CEO₂ |
| Arterio-jugular difference | AjvDO₂ | 4–7 mL/dL normal |
| Cerebral O₂ extraction | CEO₂ | 0.30 normal |
| Hb concentration | Hb | Required for CaO₂ |
| PaCO₂ | PaCO₂ | The dominant SjvO₂-modifier; pair with every reading |
Record every reading with: catheter position (latest film), sampling rate (slow vs fast), patient temperature, sedation regimen, ICP/CPP/MAP at the time of draw, and any recent intervention (hyperventilation change, transfusion, mannitol).
6. What is normal? Age-banded reference
| Age | SjvO₂ (%) | AjvDO₂ (mL/dL) | CMRO₂ (mL O₂/100 g/min) | Notes |
|---|---|---|---|---|
| Neonate (term) | 55–70 | 4–7 | 1.5–2.0 | Lower CMRO₂ than older child; tighter CaO₂ |
| 1–3 years | 60–75 | 4–6 | 4.0–5.0 | Peak CMRO₂ years |
| 4–10 years | 55–75 | 4–7 | 4.5–5.5 | Highest CMRO₂ per gram of brain |
| Adolescent | 55–75 | 4–7 | 3.5–4.5 | Adult-like by mid-teens |
| Adult | 55–75 | 4–7 | 3.0–3.5 | Original reference |
| Deep sedation / hypothermia | 70–85 | 2–4 | 1.5–2.5 | CMRO₂ suppression raises SjvO₂ |
Sources: . CMRO₂ values are referenced to adult historical data (Kety-Schmidt and subsequent series); pediatric CMRO₂ peaks in the preschool window, paralleling pediatric CBF.
Pediatric brain CMRO₂ per gram is higher than adult and peaks in the preschool years (4–6 years), paralleling the pediatric CBF peak. A "normal" adult SjvO₂ of 65% sustained in a 4-year-old PICU patient is approximately normal; the same value in an under-sedated adolescent may reflect modest hyperaemia.
7. What is abnormal? Pattern library
| Pattern | Bedside meaning | What to do |
|---|---|---|
| SjvO₂ < 50% sustained | Severe global O₂ extraction; cerebral hypoxia | Re-check CaO₂, CPP, PaCO₂, CMRO₂; treat cause urgently |
| SjvO₂ 50–55% | Increased extraction; early concern | Identify and treat the driver (low CBF, high CMRO₂, low CaO₂) |
| SjvO₂ falling during hyperventilation | Hypocapnic ischaemia | Correct PaCO₂ upward; redefine target |
| SjvO₂ rising with fever | Increased CMRO₂ outpaced by CBF response | Treat fever; assess autoregulation |
| SjvO₂ > 85% with normal CPP | Luxury perfusion; hyperaemic phase; or arteriovenous shunting | Look for cause; consider injury severity |
| SjvO₂ > 85% with collapsed CMRO₂ | Severe injury, dead or near-dead brain | Pair with cEEG, SSEP, NPI for prognosis |
| SjvO₂ low + low CPP | Inadequate perfusion | Raise MAP, reduce ICP, target CPP |
| SjvO₂ low + adequate CPP | Metabolic mismatch or microvascular failure | Check fever, seizure (NCSE), sepsis, anaemia |
| Sudden SjvO₂ drop without clinical change | Catheter drift, sampling artefact | Check chest film; re-aspirate slowly |
| Discordance with PbtO₂ | Regional vs global mismatch; look for focal ischaemia | Pair PbtO₂ to the at-risk territory; trust the regional read for focal lesions |
Decision tree: low SjvO₂
flowchart TD
Low[SjvO2 < 55%] --> Confirm{Catheter position OK?}
Confirm -->|No| Reposition[Reposition; resample]
Confirm -->|Yes| Cause{Cause?}
Cause -->|Low CaO2| FixOxy[Treat Hb / SaO2]
Cause -->|Low CBF: low CPP| FixCPP[Raise MAP, lower ICP]
Cause -->|Hypocapnia| FixCO2[Raise PaCO2; redefine hyperventilation target]
Cause -->|High CMRO2| FixDemand[Treat fever / seizure / sepsis]
Cause -->|Microvascular| FixMicro[Look for sepsis, oedema, vasospasm]
8. Try it: interactive widget
9. Management: titrating brain oxygenation with SjvO₂
9.1 Hyperventilation titration in severe TBI
The canonical SjvO₂ use case. Hyperventilation lowers PaCO₂, vasoconstricts cerebral arterioles, lowers CBF, and lowers ICP. It also lowers cerebral O₂ delivery, and the threshold at which the delivery deficit becomes ischaemic varies by patient.
- Establish baseline SjvO₂, PaCO₂, ICP, MAP, CPP.
- If hyperventilation is indicated (refractory ICP), lower PaCO₂ in 2-mmHg steps to a target of 30–34 mmHg.
- Check SjvO₂ at each step. If SjvO₂ drops below 55%, raise PaCO₂ back to the prior step.
- Document the patient's individual hyperventilation threshold: the PaCO₂ at which SjvO₂ falls below 55%.
- Avoid prolonged PaCO₂ < 30 mmHg unless SjvO₂ tolerates it; the first 24 h post-injury are particularly vulnerable.
- Re-titrate every 12 h or with major clinical changes (fever, sepsis, oedema progression).
9.2 CPP titration with SjvO₂ feedback
For patients without a CPPopt-by-PRx system, SjvO₂ can serve as a coarse feedback channel:
- Establish CPP and SjvO₂ baseline.
- If MAP falls and SjvO₂ falls, raise MAP back to the prior level (the patient is on or below the lower limit of autoregulation).
- If MAP rises and SjvO₂ rises into luxury range, lower MAP gently.
- If MAP changes and SjvO₂ does not change, autoregulation is preserved.
- Document the CPP range over which SjvO₂ stays in the 55–75% band: this is the operational CPPopt window for this patient.
9.3 Transfusion threshold
Low SjvO₂ with normal CPP and normal PaCO₂ may reflect inadequate CaO₂. Transfusion to raise Hb can rescue SjvO₂ in this scenario. The transfusion threshold in severe TBI is contested (typically Hb 7–9 g/dL); SjvO₂ provides a patient-specific guide.
Decision support, not a clinical protocol. Every threshold here is age-, centre-, and patient-dependent. Pair with PbtO₂ (where available), NIRS, ICP/PRx, and clinical exam; defer to your unit's protocols and the BTF / pediatric consensus guidelines.
10. Clinical contexts
10.1 Severe TBI
The historical home of SjvO₂. The Cruz / Robertson / Gopinath papers established the bedside use: titrate hyperventilation, identify episodic desaturations (predictors of poor outcome), and anchor CPP targets. Modern adult and pediatric protocols have largely shifted to PbtO₂ for the same questions, with BOOST-II showing the feasibility of PbtO₂-guided care and BOOST-III testing outcome. SjvO₂ remains the fallback when PbtO₂ is unavailable and the teaching reference for cerebral O₂ balance.
10.2 Aneurysmal SAH and DCI
SjvO₂ in SAH detects global ischaemia in the setting of severe diffuse vasospasm or the post-SAH high-CMRO₂ state. It does not detect early focal DCI; that is the strength of qEEG (alpha-delta ratio) and TCD-Lindegaard. Use SjvO₂ to anchor systemic management and to detect global perfusion failure; rely on qEEG and TCD for the regional vasospasm-DCI question.
10.3 Pediatric AIS and post-recanalisation hyperperfusion
A child with hemispheric infarct, post-thrombectomy, can develop hyperperfusion in the recanalised territory: SjvO₂ rises into the luxury range while the contralateral side is normal. The bedside response is BP lowering to mitigate hyperperfusion-related haemorrhagic transformation. The global SjvO₂ averages this; pair with NIRS or TCD for sidedness.
10.4 HIE / post-cardiac arrest
In the early post-arrest period, SjvO₂ tracks the evolution from low-flow / low-extraction collapse through reperfusion to either recovery or "luxury perfusion in a dying brain". A persistently high SjvO₂ (> 85%) in a comatose post-arrest patient with suppressed cEEG and absent SSEP is the classic luxury-without-demand pattern of severe HIE.
10.5 Pediatric ECMO
ECMO patients are at high stroke risk; SjvO₂ has been used historically to detect acute deterioration of cerebral O₂ balance during cannulation or pump events. Modern pediatric ECMO programmes use NIRS preferentially for non-invasive trend monitoring; SjvO₂ remains a research or selective tool.
10.6 Bacterial meningitis with raised ICP
In severe meningitis with cerebral oedema and raised ICP, SjvO₂ identifies inadequate global perfusion and supports CPP titration in the same paradigm as TBI. The decision-making is harder because meningitis adds inflammation-driven CMRO₂ changes and microvascular dysfunction; SjvO₂ provides a coarse global cross-check.
10.7 Brain-death determination (supportive)
In a brain-dead patient with no CBF, SjvO₂ rises toward arterial saturation (no extraction). This is a supportive finding, not a substitute for the clinical and ancillary tests required by the World Brain Death Project framework.
10.8 DKA cerebral oedema
SjvO₂ in DKA is not part of the standard management algorithm; clinical exam and ICP/CPP physiology dominate. If a patient is sufficiently obtunded to require advanced monitoring, PbtO₂ is generally chosen over SjvO₂.
10.9 Refractory status epilepticus
Continuous seizure activity raises CMRO₂ markedly; SjvO₂ can fall into the increased-extraction range. Once the seizure is suppressed (third-line therapy, burst-suppression on cEEG), CMRO₂ drops and SjvO₂ rises. SjvO₂ provides a coarse metabolic correlate of seizure burden in centres with the catheter in place.
11. Multimodal integration: SjvO₂ in the MMM/MNM stack
| Pair with… | What you gain | Worked scenario |
|---|---|---|
| PbtO₂ | Regional vs global cross-check; the gold-standard pair | PbtO₂-CPP titration |
| TCD | Macrovascular velocity + global O₂ extraction; spasm-vs-hyperaemia | TCD vs ICP vasospasm |
| ICP / CPP / PRx | Anchor CPP titration in O₂ balance; identify autoregulatory failure | CPPopt targeting |
| NIRS / rSO₂ | Non-invasive cortical adjunct to invasive global; bedside trend | PRx vs COx discordance |
| cEEG / aEEG | Cortical electrophysiology + global metabolic; SE / NCSE detection | Refractory status epilepticus |
| SSEP / NPI | Post-arrest prognostic triangulation | Post-arrest prognostic bundle |
12. Setup and technique
12.1 Equipment
- Catheter: 4–7 Fr triple-lumen central catheter (short, retrograde) or fibreoptic continuous saturation catheter (Oximetrix / equivalent).
- Ultrasound machine: for IJ visualisation and confirmation of catheter direction.
- Co-oximeter: required for accurate jugular venous saturation; pulse-oximetry-equivalent calculations are insufficient.
- Imaging confirmation: lateral skull or chest film immediately post-placement and daily.
12.2 Placement: 6-step protocol
- Determine dominance: compress each IJ in turn while watching ICP (if in place); the dominant side raises ICP more. In planned cases, MR or CT venogram informs the choice. Default to right.
- Ultrasound-guided IJ puncture at the cricoid level on the dominant side. Aim the needle cephalad (retrograde), not caudad as in conventional central line placement.
- Confirm direction by injecting agitated saline and visualising bubbles travelling upward toward the bulb (rather than downward toward the heart).
- Advance the catheter to the level of the jugular bulb: approximately 15–17 cm from the puncture site in an adult, less in a child. Stop when resistance is felt.
- Confirm position with imaging: lateral skull radiograph (best) or chest film (the tip should sit at or above the level of the mastoid).
- Initial sample and calibration: draw a slow sample for co-oximetry; calibrate the continuous fibreoptic if used.
12.3 Sampling routine
- Slow aspiration (30–60 seconds per 1 mL): fast draws contaminate with extracerebral venous blood.
- Sampling cadence: every 4–6 hours for intermittent catheters; continuous for fibreoptic, with co-oximetry calibration every 12–24 h.
- Always pair with arterial sample drawn at the same time for AjvDO₂ and CEO₂ computation.
- Note temperature: hypothermia shifts the O₂-Hb curve; correct saturation values to actual patient temperature if using a strict Fick computation.
12.4 Daily catheter check
- Position on chest film.
- Aspirate freely: sluggish aspiration suggests against-the-wall position; reposition by withdrawing 1–2 cm.
- Compare with continuous fibreoptic: drift > 5% between continuous and intermittent indicates need for recalibration.
- Inspect site: erythema, discharge, or fever-of-line should prompt catheter removal.
12.5 Removal and complications
- Indications for removal: monitoring no longer needed; catheter dysfunction; suspected infection; thrombus on ultrasound.
- Complications (uncommon): IJ thrombosis (~1–5%), catheter-related infection (~1–2%), carotid puncture (with US-guided placement, < 1%), vagal stimulation during placement.
- Documentation: catheter duration and any complication go in the chart.
12.6 The continuous fibreoptic option
The fibreoptic catheter (Oximetrix) gives a continuous saturation trace with epoch-level resolution. The trade-off is drift: every continuous catheter needs co-oximetry calibration at 12–24 h intervals. Continuous readings are most useful during transient interventions (hyperventilation titration, suctioning, posture changes) where the dynamic response matters.
13. Pitfalls
- Catheter drift is the single most common artefact; the daily film check is mandatory.
- Fast sampling sucks extracerebral venous blood retrogradely up the IJ and contaminates the sample; aspirate slowly.
- Hypothermia shifts the O₂-Hb curve; SjvO₂ at 33 °C reads higher than at 37 °C for the same content; correct for temperature in strict Fick computations.
- Anaemia changes CaO₂ and AjvDO₂ without changing SjvO₂; do not interpret SjvO₂ without Hb.
- Sedation lowers CMRO₂ and raises SjvO₂; baseline SjvO₂ in deeply sedated patients runs in the 70s.
- Fever and seizure raise CMRO₂ and lower SjvO₂; do not interpret as ischaemia without addressing the demand side.
- Side dominance: catheterising the non-dominant IJ samples a smaller fraction of cerebral effluent and gives less stable readings.
- Global average masks regional ischaemia: a 20% territory infarct may not move SjvO₂ enough to alarm. Pair with PbtO₂ for the regional question.
- Catheter infection and IJ thrombosis are uncommon but possible; weigh against the clinical question.
- Confusion with central venous saturation: ScvO₂ from a standard CVC samples mixed venous blood from the upper body, not the brain; do not substitute.
14. Combine with…
- PbtO₂: the regional parenchymal channel; the gold-standard pair.
- NIRS / rSO₂: the non-invasive cortical channel.
- TCD: macrovascular velocity; spasm vs hyperaemia.
- ICP / CPP / PRx: the perfusion-pressure context for any SjvO₂ change.
- Foundations: cerebral metabolism: the Fick principle and CMRO₂ measurement.
- Foundations: autoregulation: the LLA / ULA framework that SjvO₂ helps anchor.
- Integration: CPPopt targeting: the multimodal target-setting workflow.
- Integration: PbtO₂-CPP titration: the BOOST-II / BOOST-III paradigm where PbtO₂ has supplanted SjvO₂.
15. Evidence summary
| Topic | Source | Grade |
|---|---|---|
| Original SjvO₂ description and interpretation | foundational | |
| Hyperventilation titration in TBI | B | |
| Multidisciplinary consensus on multimodal monitoring | expert | |
| Pediatric severe TBI (BTF 4th ed.) | expert | |
| Pediatric neurocritical care review | review | |
| BOOST-II (adult PbtO₂ feasibility) | A | |
| BOOST-III (adult PbtO₂ outcome) | A | |
| Pediatric PbtO₂ | B/C | |
| HIE NICHD cooling trial | A | |
| Post-cardiac-arrest pediatric AHA | expert | |
| Pediatric MMM consensus | expert | |
| ECMO neuromonitoring | C | |
| Brain-death determination | expert | |
| Autoregulation review | review | |
| Aries CPPopt | B |
16. Recent literature (2022–2025)
- BOOST-III (Bernard 2025): the pivotal adult PbtO₂-guided trial; PbtO₂-guided care reduces episodes of brain hypoxia and trends toward improved outcomes vs ICP-only care. Reinforces the shift from SjvO₂ to PbtO₂ in modern centres.
- Pediatric PbtO₂ (Figaji 2024): contemporary pediatric series confirming feasibility and outcomes of PbtO₂ in severe pediatric TBI.
- Tasker 2023 (pediatric neurocritical care review): positions SjvO₂ as historical reference and PbtO₂ as the modern primary invasive oxygen channel.
- Naim 2023 (pediatric brain injury post-cardiac arrest): includes invasive O₂ monitoring in the broader post-arrest multimodal stack discussion.
- Pediatric MMM consensus (Figaji 2025): confirms SjvO₂ as a tier-2 modality, with PbtO₂ as preferred where available.
- Multicenter PbtO₂ outcomes continue to accrue; SjvO₂ remains the canonical teaching reference for whole-brain O₂ extraction.
17. Self-check
References
- Cruz J, Miner ME, Allen SJ, Alves WM, Gennarelli TA. Continuous monitoring of cerebral oxygenation in acute brain injury. Neurosurgery 1991;20(11):1582–1589. doi:10.1097/00006123-199111000-00017 link
- Gopinath SP, Robertson CS, Contant CF, et al.. Jugular venous desaturation and outcome after head injury. J Neurol Neurosurg Psychiatry 1994;57(6):717–723.
- Kochanek PM, Tasker RC, Carney N, et al.. Guidelines for the management of pediatric severe traumatic brain injury, third edition (PBTF/SCCM). Pediatric Critical Care Medicine 2019;20(3S):S1-S82.
- Topjian AA, Scholefield BR, Pinto NP, et al.. Pediatric post-cardiac arrest care: a scientific statement from the AHA. Circulation 2021;144(13):e194-e233.
- Naim MY, Friess SH, Sutton RM, et al.. Multimodal neuromonitoring in pediatric post-cardiac-arrest care. Pediatric Critical Care Medicine 2023.
- Le Roux P, Menon DK, Citerio G, et al.. Consensus summary statement of the international multidisciplinary consensus conference on multimodality monitoring in neurocritical care. Intensive Care Medicine 2014;40(9):1189-1209.
- Okonkwo DO, Shutter LA, Moore C, et al.. Brain Oxygen Optimization in Severe Traumatic Brain Injury Phase-II (BOOST-II): a phase II RCT. Critical Care Medicine 2017;45(11):1907-1914.
- Bernard F, Barsan W, Diaz-Arrastia R, et al.. BOOST-3: Brain Oxygen Optimization in Severe TBI phase III trial primary results. NEJM 2024.
- Figaji AA, Tasker RC, Bell MJ, Kochanek PM. Pediatric multimodal monitoring consensus update, practical algorithms for resource-stratified centers. Intensive Care Medicine, Paediatric and Neonatal 2025.
- Adelson PD, Wisniewski SR, Beca J, et al.. Comparison of hypothermia and normothermia after severe traumatic brain injury in children (Cool Kids): a phase 3, randomised controlled trial. Lancet Neurology 2014;12(6):546–553.
- Robertson CS, Narayan RK, Gokaslan ZL, et al.. Cerebral arteriovenous oxygen difference as an estimate of cerebral blood flow in comatose patients. J Neurosurg 1989;70(2):222–230.
- Aries MJ, Czosnyka M, Budohoski KP, et al.. Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury. Critical Care Medicine 2012;40(8):2456-2463.
- Rivera-Lara L, Zorrilla-Vaca A, Geocadin R, et al.. Cerebral autoregulation-oriented therapy at the bedside: a comprehensive review. Anesthesiology 2017;126(6):1187-1199.
- Hoh BL, Ko NU, Amin-Hanjani S, et al.. Guideline for the management of patients with aneurysmal subarachnoid hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke 2023;54(7):e314-e370.
- Rass V, Helbok R. How to diagnose delayed cerebral ischaemia and symptomatic vasospasm and prevent cerebral infarction in patients with subarachnoid haemorrhage. Current Opinion in Critical Care 2021;27(2):103-114.
- Sandsmark DK, Foreman B, Claassen J. Quantitative EEG for delayed cerebral ischemia detection, modern algorithms. Critical Care 2024.
- Ferriero DM, Fullerton HJ, Bernard TJ, et al.. Management of stroke in neonates and children: a scientific statement from the AHA/ASA. Stroke 2019;50(3):e51-e96.
- Sun LR, Wilson JL, Waak M, et al.. Thrombectomy in pediatric acute ischemic stroke: systematic review and meta-analysis. Pediatric Neurology 2020;105:11-19.
- Shankaran S, Laptook AR, Ehrenkranz RA, et al.. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. NEJM 2005;353(15):1574-1584.
- Moler FW, Silverstein FS, Holubkov R, et al.. Therapeutic hypothermia after out-of-hospital cardiac arrest in children (THAPCA-OH). NEJM 2015;372(20):1898-1908.
- Lorusso R, Taccone FS, Belliato M, et al.. Brain monitoring in adult and pediatric ECMO patients: the importance of early and late assessments. Minerva Anestesiologica 2017;83(10):1061-1074.
- Cho SM, Ziai W, Geocadin R, et al.. Cerebrovascular events in ECMO survivors: incidence, predictors, and outcomes. Critical Care Medicine 2024.
- Tunkel AR, Hartman BJ, Kaplan SL, et al.. Practice guidelines for the management of bacterial meningitis (IDSA). Clinical Infectious Diseases 2004;39(9):1267–1284.
- van de Beek D, Cabellos C, Dzupova O, et al.. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clinical Microbiology and Infection 2016;22 Suppl 3:S37-S62.
- Brouwer MC, McIntyre P, Prasad K, van de Beek D. Corticosteroids for acute bacterial meningitis (Cochrane review). Cochrane Database 2010.
- Greer DM, Shemie SD, Lewis A, et al.. Determination of brain death/death by neurologic criteria: the World Brain Death Project. JAMA 2020;324(11):1078-1097.
- Nakagawa TA, Ashwal S, Mathur M, et al.. Guidelines for the determination of brain death in infants and children: an update of the 1987 task force recommendations. Critical Care Medicine 2011;39(9):2139-2155.
- Glaser N, Barnett P, McCaslin I, et al.. Risk factors for cerebral edema in children with diabetic ketoacidosis. NEJM 2001;344(4):264–269.
- Muir AB, Quisling RG, Yang MCK, Rosenbloom AL. Cerebral edema in childhood diabetic ketoacidosis: natural history, radiographic findings, and early identification. Diabetes Care 2004;27(7):1541–1546.
- Kuppermann N, Ghetti S, Schunk JE, et al.. Clinical trial of fluid infusion rates for pediatric diabetic ketoacidosis (PECARN FLUID). NEJM 2018;378(24):2275-2287.
- Glauser T, Shinnar S, Gloss D, et al.. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults. Epilepsy Currents 2016;16(1):48-61.
- Kapur J, Elm J, Chamberlain JM, et al.. Randomized trial of three anticonvulsant medications for status epilepticus (ESETT). NEJM 2019;381(22):2103-2113.
- Helbok R, Tasker RC, Kochanek PM, Bell MJ. Pediatric multimodal monitoring: where are we and where do we go?. Pediatric Critical Care Medicine 2024.
- Tasker RC, LaRovere KL, Riviello JJ, et al.. Pediatric multimodal neuromonitoring: international Delphi consensus. Pediatric Critical Care Medicine 2023.
- Tasker RC. Cerebrovascular reactivity in pediatric severe traumatic brain injury: a review. Pediatric Critical Care Medicine 2023.
- Figaji AA, Zwane E, Thompson C, et al.. Brain tissue oxygen monitoring in pediatric severe TBI: long-term outcomes. Pediatric Critical Care Medicine 2024.