Near-infrared spectroscopy (NIRS)
Cerebral oximetry by light, transcutaneous regional saturation 2–3 cm below the optode, plus an autoregulation index (COx) that needs only an arterial line. Pediatric-first.
1. Bedside vignettes: why this matters in the PICU
Vignette A. CHD on bypass, rSO2 crashes during arch reconstruction
A 6-month-old undergoing Norwood-stage arch reconstruction on cardiopulmonary bypass. Pre-bypass baseline rSO2 72% bilaterally. On selective antegrade cerebral perfusion during arch repair, the left rSO2 drops to 45% and the right to 58%, asymmetric. The perfusionist increases pump flow, the surgeon adjusts the cannula, and the rSO2 returns to 65% within 90 seconds. Without NIRS, the asymmetry would not have been detected; the left-arm reading might have remained "acceptable" because cerebral perfusion was selectively compromised. Post-op MRI at day 5 shows no new ischaemic lesions. The intra-operative NIRS trend changed surgical decisions in real time.
Vignette B. Preterm 28-weeker, SafeBoosC algorithm
A 28-week preterm in the NICU, day 1. NIRS rSO2 oscillating between 40 and 55%, time below 55% accumulating at ~25% of monitored time. The SafeBoosC III algorithm fires: confirm signal, check FiO2 and arterial saturation, check Hb (transfuse if < 11), check MAP (lift if below age-appropriate), check PaCO2 (avoid hypocapnia). The team transfuses for a haemoglobin of 9.5 and raises FiO2 from 0.21 to 0.25; rSO2 stabilises at 65%. The full SafeBoosC III trial showed no overall difference in death or severe brain injury, but a per-protocol analysis suggested benefit in the subset where the algorithm was strictly applied.
Vignette C. PICU septic shock, rSO2 falls despite stable BP
A 5-year-old in septic shock day 1, MAP 65 (above the age-adjusted target), on noradrenaline 0.3 mcg/kg/min. The bedside NIRS shows rSO2 declining from 68% on admission to 52% over 6 hours, despite stable MAP and lactate falling. COx has become positive (+0.35) suggesting impaired cerebral autoregulation. The team interprets this as the start of microcirculatory failure: macroscopic perfusion looks fine but tissue oxygenation is suffering. They escalate to MAP target 75 (per noradrenaline titration), and rSO2 stabilises at 60%; COx falls to +0.10. NIRS detected what BP-only monitoring missed.
2. What NIRS is, and what it is not
NIRS is continuous transcutaneous cerebral oximetry based on the modified Beer-Lambert law: light at two wavelengths is differentially absorbed by oxygenated (HbO) and deoxygenated (HbR) haemoglobin, and the ratio gives saturation.
Two wavelengths are typical: ~730 nm (peak HbR absorption) and ~810 nm (isobestic). Modern devices use 4 wavelengths plus algorithms to reduce extracerebral contamination via the near-far detector subtraction (the near detector samples scalp/skull, the far detector samples scalp/skull + cortex; the difference is the cortical sample).
What rSO2 represents. A 2–3 cm "banana-shaped" cortical sample under the optode, weighted approximately 75% venous, 25% arterial. This is not a global brain measurement; it is a frontal-cortical regional sample. With bilateral optodes, the asymmetry is itself a clinical signal.
Two things follow.
NIRS measures regional, not global. A unilateral MCA occlusion will produce ipsilateral rSO2 drop without changing the contralateral side. Bilateral optodes are essential whenever the lesion can be unilateral.
NIRS is venous-weighted. rSO2 falls when tissue extracts more O2 (rising CMRO2 with stable supply) or when delivery falls (low CBF, low SaO2, low Hb). It does not separate these causes; pair with TCD (delivery), PbtO2 (tissue), and EEG (demand).
Trend, not absolute. Baseline rSO2 varies by device (INVOS, Foresight, Masimo, EQUANOX read different absolute numbers on the same patient), by age, by Hb, and by skin pigmentation. The clinically useful number is fractional change from baseline and time below threshold.
Pediatric rSO2 norms are age-dependent. Term newborns sit at 70–80% (high baseline due to lower CMRO2). Preterm neonates 70–90% in the first 72 hours, falling as the brain matures. Older children and adolescents 65–75% on most modern devices. The SafeBoosC threshold of 55% (intervention target) and 55–85% target range for preterms is the most validated pediatric specific threshold.
3. Optode placement and physics
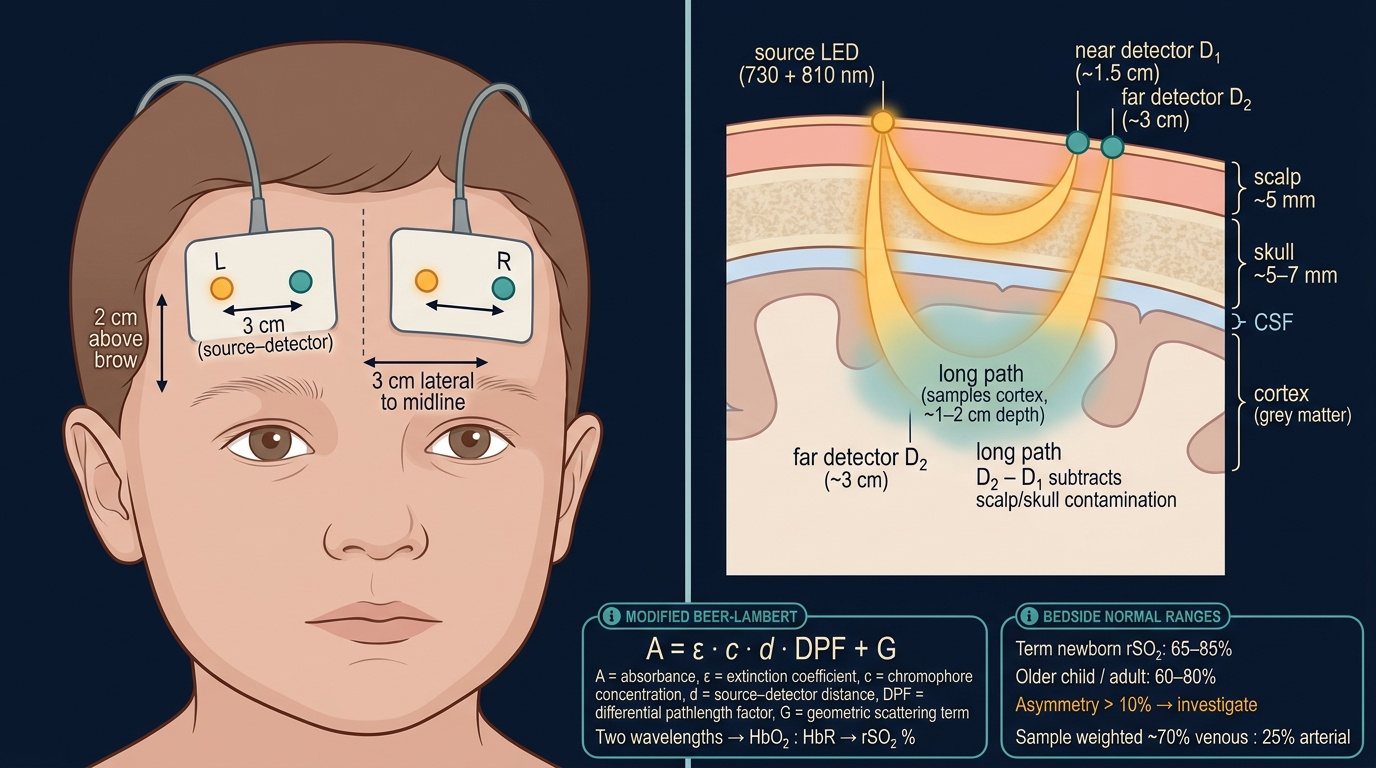
Optode placement. Standard frontal placement: 2 cm above each eyebrow, 3 cm lateral to midline. This samples frontal cortex bilaterally. Some protocols add a third optode (occipital or temporal) for monitoring posterior circulation in specific contexts.
Skin prep. Clean, dry, intact skin. Hair under the optode falsifies the signal; shave or use a tight optode contact. Skin pigmentation slightly biases the absolute number (darker skin reads ~2–5% lower on some devices) but trends are reliable across pigmentation.
Light shielding. Ambient light (especially halogen, fluorescent, and sunlight) interferes with the detector. Light-tight covers are standard.
Sample volume. The 2–3 cm penetration depth limits NIRS to cortical sampling. Deep grey matter (basal ganglia, thalamus) and brainstem are not sampled.
4. The numbers: what to record and in what order
For every patient, on every shift, record this six-pack:
| Variable | What it tells you | Bedside use |
|---|---|---|
| rSO2 (left, right) | Regional cortical oxygenation | Primary number; trend per shift |
| Fractional change from baseline | Δ rSO2 / baseline | More informative than absolute; alert at > 20% drop |
| Time below threshold | Minutes with rSO2 < 50% (or 40% preterm) | Dose-response analogue; outcome-mapped |
| COx | Correlation (rSO2, MAP) | Autoregulation index, non-invasive |
| Asymmetry | abs(left − right) | > 10% suggests unilateral pathology |
| Variability | Standard deviation over 1 h | High variability suggests sensor problem or vasomotor instability |
Why time-below-threshold matters. In adult cardiac surgery, NIRS-guided intervention reduces stroke and cognitive decline when time below 80% of baseline is treated. In neonatal CHD, time below 50% predicts MRI injury. In preterm SafeBoosC, time below 55% is the algorithm trigger. The pediatric severe-TBI literature (Davies 2017) uses time below 50% as a comparable threshold.
5. What is normal? Age-banded reference values
| Age | rSO2 baseline range | Action threshold |
|---|---|---|
| Preterm 24–32 wk | 70–90% | < 55% (SafeBoosC algorithm) |
| Term newborn (< 7 d) | 70–80% | < 50% or > 20% drop from baseline |
| Infant 1–11 mo | 65–80% | < 50% or > 20% drop |
| Toddler 1–3 y | 65–78% | < 50% |
| Child 4–11 y | 65–75% | < 50% |
| Adolescent 12–18 y | 60–75% | < 50% |
| Adult reference | 60–75% | < 50% or 20% drop from baseline |
Sources: .
Device-specific differences matter. INVOS reads ~5% lower than Foresight on the same patient. Masimo O3 and EQUANOX have their own calibration curves. Within a single patient on a single device, the trend is the clinically useful signal; across devices and across patients, absolute comparisons are unreliable.
SafeBoosC framework: the most validated pediatric NIRS algorithm. Designed for preterm neonates (24–32 weeks). Targets rSO2 between 55 and 85%; algorithm triggers escalating interventions for time below or above the band. SafeBoosC II (proof-of-concept, 2015) showed feasibility; SafeBoosC III (2023, ~1600 preterms) showed no overall benefit on death or severe brain injury but per-protocol analysis suggested benefit in centres with strict adherence.
6. What is abnormal? A pattern library
| Pattern | Bedside meaning | What to do |
|---|---|---|
| Stable baseline 65–75% | Normal cortical perfusion | Continue monitoring |
| Bilateral drop > 20% from baseline | Hypoperfusion, hypoxia, or low Hb | Check MAP, SaO2, Hb, CO2; treat accordingly |
| Bilateral rise to 80–90% | Hyperaemia (post-arrest luxury, fever, vasodilator) | Investigate; pair with EEG and TCD |
| Asymmetric (> 10% difference) | Unilateral pathology (MCA occlusion, selective perfusion, sensor migration) | Confirm with imaging; check optode placement |
| COx > +0.3 sustained | Impaired autoregulation | Re-target MAP per COxopt where available |
| Jumpy trace with poor coupling | Sensor artefact, hair, ambient light | Reposition, replace optode |
| rSO2 < 50% sustained | Cerebral hypoxia regardless of cause | Acute action: airway, breathing, circulation, transfusion |
| rSO2 sustained > 85% in HIE / post-arrest | Luxury perfusion pattern: bad prognosis | Pair with EEG; counsel family |
7. Try it: interactive widgets
8. BP / CPP management with COx
COx (cerebral oximetry index) is the slow-wave correlation between rSO2 and MAP, computed over the same 5-minute window as PRx.
Interpretation. When autoregulation is intact, rSO2 is stable across MAP changes (the cortex compensates for delivery changes via vasomotor tone). COx is near zero or negative. When autoregulation is impaired, rSO2 follows MAP passively. COx becomes positive (> +0.3 indicates impairment).
8.1 COxopt: the NIRS-only individualised target
The same parabolic fit logic as PRx-CPPopt applies. Plot (MAP, COx) over the past 4 hours, fit a parabola, the vertex is MAPopt (since CPP cannot be computed without ICP). Pediatric piglet validation (Brady 2007, 2009) established the framework; adult and limited pediatric clinical data extend it. COx-derived autoregulation is particularly valuable in:
- VA-ECMO where PRx is uninterpretable.
- Cardiac surgery during and after bypass.
- Severe TBI without invasive ICP placed.
- Pediatric stroke / thrombectomy post-procedure.
8.2 The SafeBoosC neonatal algorithm
The SafeBoosC framework for preterms uses a structured intervention algorithm when rSO2 drops below or rises above the 55–85% target band. Each branch addresses a candidate cause:
flowchart TD
Read[rSO2 below 55 percent] --> Signal{Signal good?}
Signal -->|No| Reposition[Reposition optode]
Signal -->|Yes| O2{SaO2 below 90?}
O2 -->|Yes| FiO2[Increase FiO2 toward target]
O2 -->|No| Hb{Hb below 11?}
Hb -->|Yes| Trans[Transfuse]
Hb -->|No| MAP{MAP below target?}
MAP -->|Yes| Pressure[Lift MAP per protocol]
MAP -->|No| CO2{PaCO2 below 35?}
CO2 -->|Yes| Vent[Adjust ventilation toward normocapnia]
CO2 -->|No| Seizure[Consider EEG; investigate]
Decision support, not a clinical protocol. Every threshold and intervention above is context-dependent. Defer to your unit's protocols and senior clinical team.
9. Clinical contexts: NIRS across acute brain injuries and surgical contexts
9.1 Congenital heart disease (intra-operative and ICU)
The most validated adult-equivalent context. Multiple studies show NIRS-guided intra-operative care reduces:
- Stroke and cognitive decline in adult cardiac surgery (small RCTs and observational).
- Adverse neurological events in pediatric Norwood-stage palliation (selective antegrade perfusion monitoring).
- Time below threshold predicts MRI brain injury at day 5–7 post-op.
The Brain Injury in Children with Congenital Heart Disease consensus (Naim 2023) endorses bilateral NIRS as standard intra-operative and early post-operative monitoring in complex CHD.
9.2 Preterm neonates (SafeBoosC framework)
SafeBoosC II (2015, ~166 preterms, feasibility) showed the algorithm could be implemented and reduced time outside the target band. SafeBoosC III (2023, ~1600 preterms, definitive trial) showed no overall benefit on death or severe brain injury at 36 weeks postmenstrual age. Per-protocol and post-hoc analyses suggested benefit in subgroups with strict algorithm adherence. The framework remains in clinical use but is not endorsed as routine standard of care universally.
9.3 Septic shock
NIRS in pediatric septic shock detects microcirculatory failure earlier than BP or lactate alone. A falling rSO2 with stable MAP suggests vasodilatory shock with maintained macroperfusion but impaired tissue extraction. The COx becoming positive in shock is a marker of autoregulation failure.
9.4 Severe TBI (adult and pediatric)
NIRS in severe TBI is less validated than ICP but provides regional cortical monitoring. Davies 2017 review summarises NIRS use in TBI; the modality is most useful when ICP is contraindicated (coagulopathy, hepatic failure), as a non-invasive autoregulation surrogate via COx, and for early triage. Pediatric MNM consensus 2025 includes NIRS as tier-2 modality in resource-stratified pediatric centres.
9.5 Cardiac arrest and ROSC monitoring
NIRS has emerged as a real-time CPR quality marker: rising rSO2 during compressions predicts ROSC; falling rSO2 predicts failure. Post-arrest, the rSO2 trend pairs with EEG: rSO2 rising > 85% with isoelectric EEG signals luxury perfusion and poor prognosis.
9.6 Pediatric arterial ischaemic stroke and thrombectomy
NIRS during thrombectomy provides bilateral cortical monitoring. Sun 2020 pediatric thrombectomy cohort and Ferriero 2019 AHA pediatric stroke statement endorse NIRS as adjunctive monitoring where available, especially post-recanalisation when reperfusion injury is a risk.
9.7 SAH and DCI (limited validation)
NIRS in SAH is less established than TCD. The principle (regional cortical oxygenation as a DCI early-warning) is sound but evidence base is single-centre. Some centres use combined NIRS-TCD as a "non-invasive DCI bundle" alongside clinical exam. Sparse
9.8 ECMO
NIRS in ECMO is highly valuable because PRx is uninterpretable in non-pulsatile flow. Bilateral rSO2 + COx + TCD-asymmetry monitoring detect cerebral perfusion failure days before clinical signs. Cho 2024 pediatric ECMO outcomes review supports NIRS as standard ECMO neurological monitoring; ELSO 2017 consensus endorses adjunctive use.
10. Multimodal integration: NIRS in the MMM/MNM stack
| Pair with… | What you gain | Worked scenario |
|---|---|---|
| TCD | Macro (large-vessel velocity) + micro (cortical saturation) | TCD page |
| PbtO2 | Regional non-invasive surrogate + invasive gold standard | PbtO2 page |
| EEG / aEEG | Cortical activity vs cortical oxygenation, reactivity loss in HIE | EEG page |
| PRx | Cross-validate autoregulation (COx vs PRx); discordance is information | PRx page |
| CPPopt / COxopt | Individualised perfusion target via NIRS alone | CPPopt page |
| Pupillometry | Brainstem function alongside cortical oxygenation | Pupillometry page |
| ICP | Tissue oxygenation paired with invasive pressure | ICP page |
| Clinical exam | Most important pairing; rSO2 in isolation can mislead | Always |
The NIRS-TCD non-invasive autoregulation bundle: combine forehead NIRS (COx) with continuous TCD-MFV (Mx) for autoregulation surveillance without an invasive ICP monitor. Useful in pediatric severe TBI pre-ICP placement and in any patient where invasive monitoring is contraindicated.
11. Setup and technique: a step-by-step
11.1 Optode selection
Choose the device that matches the patient size and the clinical context:
- Neonatal optodes (small, low-power, transcranial-friendly for thin scalps).
- Pediatric optodes (medium size, calibrated for age 1+).
- Adult optodes (standard adult forehead size).
Devices: INVOS (Covidien/Medtronic), Foresight (Casmed), Masimo O3, EQUANOX (Nonin). All produce regional rSO2 but absolute numbers differ by ~5–10% between devices on the same patient. Within-patient trends are reliable; cross-device comparison is not.
11.2 Placement
- Frontal placement: 2 cm above eyebrow, 3 cm lateral to midline. Bilateral.
- Avoid the sinuses: ethmoid/frontal sinuses produce signal voids in older children and adults.
- Avoid hair: shave or use hair-free site; hair under optode falsifies signal.
- Skin condition: intact, clean, dry skin. Skin lesions or pigmentation variation can bias the absolute number but not the trend.
11.3 Light shielding
Ambient light at the optode causes artefact. Light-tight covers come with most devices; some pediatric NICU/PICU rooms use additional opaque drapes during phototherapy.
11.4 Inter-device calibration
INVOS, Foresight, Masimo, and EQUANOX use proprietary algorithms and read different absolute rSO2 on the same patient. When comparing across studies or across patients monitored on different devices, use the fractional change from baseline or time below threshold rather than absolute number.
11.5 Continuous monitoring during procedures
NIRS is standard for:
- Pediatric cardiac surgery (intra-op and 24 h post-op).
- ECMO (continuous duration of run).
- Severe TBI in PICU (continuous duration of monitoring).
- Preterm neonates per SafeBoosC algorithm.
11.6 Hair, skin pigmentation, and other physical confounders
- Hair under optode: shave or use hair-free placement.
- Skin pigmentation: darker skin tones may read 2–5% lower on some devices; trends are reliable.
- Skin lesions, scalp haematomas: avoid placement over lesions; choose alternative site.
- Cephalohaematoma in newborns: avoid the site; choose the unaffected side.
12. Pitfalls and artefacts
- Extracerebral contamination: scalp blood flow contributes to the signal; modern multi-distance optodes minimise but do not eliminate this.
- Sensor migration: a slipped optode shows as sudden rSO2 change without clinical correlate. Verify placement physically.
- Low arterial saturation paradoxes: profound hypoxaemia can produce paradoxical rSO2 readings on some devices.
- Calibration drift: long-duration monitoring (> 7 days) may drift; re-baseline if the device offers it.
- Anaemia: low Hb reduces total chromophore concentration; rSO2 may read lower at the same true tissue oxygenation.
- Skin pigmentation: small bias on absolute number; reliable trends.
- Optode placement variability: even small (2 cm) shifts in placement change the sampled cortical region.
- Ambient light: halogen, fluorescent, and sunlight interfere; use light shields.
- CPR motion: chest compressions produce massive artefact; rSO2 during CPR is interpreted with caution.
- Device cross-comparison: never compare absolute rSO2 across INVOS / Foresight / Masimo / EQUANOX.
13. Combine with…
- Advanced NIRS: frequency-domain, time-resolved, broadband.
- COx: the NIRS-based autoregulation index.
- PRx: the invasive autoregulation comparator.
- TCD: for the non-invasive autoregulation bundle.
- PbtO2: the invasive tissue-oxygenation gold standard.
- SjvO2: the global cerebral oxygenation comparator.
- CPPopt: for the individualised perfusion target.
- EEG: for reactivity + oxygenation pairing.
- Pupillometry: for brainstem function alongside cortical oxygenation.
14. Evidence summary and recent literature
14.1 Evidence summary
| Topic | Source | Grade |
|---|---|---|
| Original NIRS description | foundational | |
| Kirkpatrick 1995, intra-op validation | B | |
| Madsen 2000, neonatal NIRS | B | |
| Hyttel-Sorensen 2015 SafeBoosC II | A | |
| Hansen 2023 SafeBoosC III | A | |
| Plomgaard 2024 SafeBoosC III analysis | A | |
| Kurth 2009 pediatric CHD reference | B | |
| Davies 2017 NIRS in TBI review | review | |
| Andresen 2014 NIRS critical care | review | |
| Lee 2009 ND NIRS | B | |
| Brady 2010 COx | B | |
| Rivera-Lara 2017 autoregulation methods | review | |
| Naim 2023 brain injury in pediatric CHD | expert | |
| Toet 2002 NIRS in HIE | C | |
| Greisen 2018 NIRS review | review | |
| Pediatric MNM consensus 2025 | expert | |
| NCS MMM consensus | expert |
14.2 Recent literature (2022–2025)
- SafeBoosC III (Hansen 2023, Plomgaard 2024): the largest pediatric NIRS RCT. No overall benefit on primary outcome at 36 weeks; per-protocol analyses suggest benefit with strict algorithm adherence. The framework remains in clinical use; standard of care remains centre-dependent.
- Naim 2023 PCCM brain injury in CHD review: synthesises NIRS evidence in pediatric cardiac care; endorses bilateral NIRS as standard intra-op and early ICU monitoring.
- Figaji 2025 Pediatric MNM consensus: NIRS as tier-2 modality in resourced pediatric centres; primary value in pediatric severe TBI pre-ICP placement and in any patient where invasive monitoring is contraindicated.
- Cho 2024 pediatric ECMO outcomes: NIRS-driven neurological surveillance on ECMO; rising adoption.
- Rivera-Lara 2017 autoregulation review: contemporary methodological reference for COx alongside PRx and Mx.
- COxopt and MAPopt extensions: NIRS-only individualised targets validated in pediatric piglet (Brady 2007, 2009) and emerging in adult cardiac surgery; pediatric clinical validation pending.
15. Self-check
References
- Kurth CD, McCann JC, Wu J, Miles L, Loepke AW. Cerebral oxygen saturation-time threshold for hypoxic-ischemic injury in piglets. Anesthesia & Analgesia 2009;108(4):1268–1277. doi:10.1213/ane.0b013e318196ac8e link
- Naim MY, Friess SH, Sutton RM, et al.. Multimodal neuromonitoring in pediatric post-cardiac-arrest care. Pediatric Critical Care Medicine 2023.
- Hyttel-Sørensen S, Pellicer A, Alderliesten T, et al. (SafeBoosC Trial Group). Cerebral near infrared spectroscopy oximetry in extremely preterm infants: phase II randomised clinical trial. BMJ 2015;350:g7635.
- Hansen ML, Pellicer A, Hyttel-Sørensen S, et al. (SafeBoosC-III Trial Group). Cerebral oximetry monitoring in extremely preterm infants. NEJM 2023;388(16):1501–1511. doi:10.1056/NEJMoa2207554 link
- Plomgaard AM, Hyttel-Sørensen S, Greisen G. SafeBoosC-III: NIRS oximetry-guided management in extremely preterm infants, five-year follow-up. Lancet Child & Adolescent Health 2024.
- Brady KM, Lee JK, Kibler KK, et al.. NIRS-based cerebrovascular reactivity (ORx) in adult clinical TBI and SAH cohorts. Neurocritical Care 2010.
- Andresen B, Greisen G, Hyttel-Sorensen S. Comparison of INVOS 5100C and Nonin SenSmart X-100 oximeter performance in preterm infants with spontaneous apnea. Pediatric Research 2014;79:466-472.
- Rivera-Lara L, Zorrilla-Vaca A, Geocadin R, et al.. Cerebral autoregulation-oriented therapy at the bedside: a comprehensive review. Anesthesiology 2017;126(6):1187-1199.
- Davies DJ, Su Z, Clancy MT, et al.. Near-infrared spectroscopy in the monitoring of adult traumatic brain injury: a review. Journal of Neurotrauma 2015;32(13):933-941.
- Brady KM, Lee JK, Kibler KK, et al.. Continuous measurement of autoregulation by spontaneous fluctuations in cerebral perfusion pressure: comparison of 3 methods. Stroke 2007;38(11):2818–2825.
- Brady KM, Mytar JO, Lee JK, et al.. Brain-induced hyperemia: a piglet model of cerebral autoregulation. Anesthesiology 2009.
- Lee JK, Kibler KK, Benni PB, et al.. Cerebrovascular reactivity measured by near-infrared spectroscopy. Stroke 2009;40(5):1820-1826.
- Figaji AA, Tasker RC, Bell MJ, Kochanek PM. Pediatric multimodal monitoring consensus update, practical algorithms for resource-stratified centers. Intensive Care Medicine, Paediatric and Neonatal 2025.
- Le Roux P, Menon DK, Citerio G, et al.. Consensus summary statement of the international multidisciplinary consensus conference on multimodality monitoring in neurocritical care. Intensive Care Medicine 2014;40(9):1189-1209.
- Topjian AA, Scholefield BR, Pinto NP, et al.. Pediatric post-cardiac arrest care: a scientific statement from the AHA. Circulation 2021;144(13):e194-e233.
- Moler FW, Silverstein FS, Holubkov R, et al.. Therapeutic hypothermia after out-of-hospital cardiac arrest in children (THAPCA-OH). NEJM 2015;372(20):1898-1908.
- Sun LR, Wilson JL, Waak M, et al.. Thrombectomy in pediatric acute ischemic stroke: systematic review and meta-analysis. Pediatric Neurology 2020;105:11-19.
- Ferriero DM, Fullerton HJ, Bernard TJ, et al.. Management of stroke in neonates and children: a scientific statement from the AHA/ASA. Stroke 2019;50(3):e51-e96.
- Rass V, Helbok R. How to diagnose delayed cerebral ischaemia and symptomatic vasospasm and prevent cerebral infarction in patients with subarachnoid haemorrhage. Current Opinion in Critical Care 2021;27(2):103-114.
- Hoh BL, Ko NU, Amin-Hanjani S, et al.. Guideline for the management of patients with aneurysmal subarachnoid hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke 2023;54(7):e314-e370.
- Cho SM, Ziai W, Geocadin R, et al.. Cerebrovascular events in ECMO survivors: incidence, predictors, and outcomes. Critical Care Medicine 2024.
- Lorusso R, Taccone FS, Belliato M, et al.. Brain monitoring in adult and pediatric ECMO patients: the importance of early and late assessments. Minerva Anestesiologica 2017;83(10):1061-1074.
- Jöbsis FF. Noninvasive infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science 1977;198(4323):1264–1267. doi:10.1126/science.929199 link
- Kirkpatrick PJ, Smielewski P, Czosnyka M, Menon DK, Pickard JD. Near-infrared spectroscopy use in patients with head injury. Journal of Neurosurgery 1995;83(6):963–970. doi:10.3171/jns.1995.83.6.0963 link
- Madsen PL, Secher NH. Near-infrared oximetry of the brain. Progress in Neurobiology 1999;58(6):541–560. doi:10.1016/s0301-0082(98)00093-8 link
- Hyttel-Sørensen S, Pellicer A, Alderliesten T, et al.. Cerebral near infrared spectroscopy oximetry in extremely preterm infants: phase II randomised clinical trial. BMJ 2015;350:g7635. doi:10.1136/bmj.g7635 link
- Toet MC, Hellström-Westas L, Groenendaal F, Eken P, de Vries LS. Amplitude integrated EEG 3 and 6 hours after birth in full term neonates with hypoxic-ischaemic encephalopathy. Archives of Disease in Childhood. Fetal and Neonatal Edition 1999;81(1):F19–23. doi:10.1136/fn.81.1.f19 link
- Greisen G. Cerebral oximetry in preterm infants, to use or not to use, that is the question. Frontiers in Pediatrics 2021;6:376. doi:10.3389/fped.2021.747660 link
- Helbok R, Tasker RC, Kochanek PM, Bell MJ. Pediatric multimodal monitoring: where are we and where do we go?. Pediatric Critical Care Medicine 2024.