Intracranial pressure monitoring
The bedrock of pediatric neurocritical care: direct measurement of the pressure inside the skull, plus the waveform that tells you whether the brain still has compensation left.
1. Bedside vignettes: why this matters in the PICU
Vignette A. Severe pediatric TBI day 1, the waveform changes shape before the number does
A 4-year-old falls from a third-floor balcony. GCS 5 on arrival; CT shows bifrontal contusions, a small subdural, and effacement of the basal cisterns. A right frontal Camino is placed within the hour; baseline ICP 14 mmHg, clean three-peak P1 > P2 > P3 waveform. By hour 18 the mean has crept to 28 mmHg sustained, and the waveform morphology has flipped: P2 > P1, rounded contour, RAP 0.8. You start the tiered escalation: head-up to 30 degrees, propofol bolus and increase infusion, hypertonic saline 3% at 3 mL/kg, normothermia, normocapnia. ICP falls to 22 over 30 minutes. The team begins to plan early decompressive craniectomy because compliance is gone, not because the absolute number is alarming.
Vignette B. Neonate with hydrocephalus, no invasive monitor available
A 3-week-old with congenital aqueductal stenosis presents with a tense, bulging anterior fontanelle, sun-set sign, and head circumference crossing two centiles in 10 days. The neurosurgeon is two hours away. There is no ICP monitor on the unit. You scan ONSD bedside: 5.8 mm bilaterally (well above the 4.0 mm pediatric cutoff for under-1s), TCD-PI 1.6 with low diastolic flow, NIRS rSO2 falling from 70 to 58%. The clinical and non-invasive picture converges on raised ICP without ever placing an invasive monitor. The infant is intubated, head elevated, and transferred for emergent third ventriculostomy.
Vignette C. Adolescent SAH day 6, EVD draining 5 mL/h, but TCD MFV is rising
A 12-year-old with a ruptured posterior-communicating aneurysm post-clipping, day 6. EVD set to drain at 10 cm H2O, mean ICP 8 mmHg, output 5 mL/h. The bedside nurse notes the right MCA TCD MFV has risen from 95 to 160 cm/s over 12 hours, with a Lindegaard ratio of 3.8. The team asks the question that ICP alone cannot answer: is this vasospasm or rising ICP? The ICP trace is reassuring; the EVD is patent (good pulsatility, respiratory swing of 2 mmHg); the TCD signature with LR > 3 is classic vasospasm. The team escalates haemodynamics (lift MAP, induce mild hypertension), schedules angiography, and the ICP trace remains stable while the spasm is treated. The ICP measured what ICP measures, and the TCD answered what the ICP could not.
2. What ICP is, and what it is not
ICP is the pressure of the supratentorial CSF + parenchymal compartment transmitted to a probe inside the skull, in mmHg. The reading reflects three superimposed signals:
- The mean, set by total intracranial volume against cranial compliance (the Monro-Kellie doctrine, Marmarou exponential P-V curve). The mean is the number nurses chart and physicians act on.
- The pulse amplitude (AMP), transmitted from the arterial pulse and modulated by compliance. AMP rises as compliance falls, often before the mean ICP does.
- The respiratory swing, transmitted from intrathoracic pressure through the venous compartment. A 1–4 mmHg swing confirms catheter patency.
The Monro-Kellie equation is the ground truth:
Once compensation is exhausted, the Marmarou exponential becomes the dominant truth:
where PVI (pressure-volume index) is the volume change that would multiply ICP by ten. PVI in healthy adults ~25 mL; in severe TBI it falls to ~10–15 mL, and the next +1 mL of oedema can double the ICP.
ICP equals brain-tissue pressure only when the waveform shape is healthy and the probe is communicating with the whole intracranial volume. In compartmentalised oedema (e.g., temporal lobe contusion behind a closed tentorium), the regional pressure can be much higher than the supratentorial probe reads. This is the canonical "ICP is normal but the pupil blew" presentation.
What ICP cannot do. It cannot localise the lesion, distinguish vasogenic from cytotoxic oedema, confirm whether autoregulation is intact, detect non-convulsive seizures driving the rise, or tell you the perfusion delivered to the tissue. It is the bedrock, not the building.
The waveform shape matters more than the number once ICP is high. P2 > P1 with RAP > 0.6 on a mean ICP of 18 is more dangerous than a clean P1-dominant trace at 28: the first is on the steep limb of the Marmarou exponential, the second is on the flat one.
Open fontanelles change the rules. Anterior fontanelle closes 12–18 months, posterior at ~2–3 months. While open, the cranium is not a closed box: the Monro-Kellie steep segment is shifted right and pressure transmission to a parenchymal probe is dampened by the compliant fontanelle. Standard adult thresholds (> 20 mmHg) under-estimate compensated raised ICP in infants. A "normal" reading in an infant with a tense, bulging fontanelle is suspicious, not reassuring. Pair every infant ICP reading with fontanelle palpation, head-circumference trajectory, ONSD, and bedside cranial ultrasound.
3. EVD versus intraparenchymal: choosing the probe
| Feature | EVD (intraventricular) | IPM (intraparenchymal) |
|---|---|---|
| Accuracy | Gold standard (fluid-coupled, re-zeroable) | Good initially, drifts ~1–3 mmHg/day |
| Drainage | Yes (therapeutic CSF removal) | No |
| CSF sampling | Yes | No |
| Bleed risk | ~5–7% (any size); ~0.5–1% clinically significant | ~1–2% |
| Infection risk | ~5–10% over 7 days (rises after day 5) | ~1% |
| Insertion difficulty | Harder (must cannulate ventricle; slit ventricles fail ~5%) | Easier (white-matter target) |
| Re-zero in situ | Yes (any time, at tragus) | No (one-shot, pre-insertion) |
| Best for | Communicating hydrocephalus, IVH, SAH with EVD indication | Diffuse TBI, slit ventricles, contraindication to ventriculostomy |
| Trend over days | Stable | Drift dominates after day 5 |
The decision tree. Choose EVD when you want to drain CSF (communicating hydrocephalus, IVH, SAH with hydrocephalus, neuro-deterioration with raised ICP and patent ventricles). Choose IPM when ventricles are slit or unavailable, when coagulopathy raises bleed concern with deeper catheter passes, or when fast bedside placement is the priority. Many units default to EVD for SAH and to IPM for diffuse TBI.
An open EVD continuously zeroes ICP to the drainage chamber height. You cannot read true ICP while the drain is open. Many units alternate drain for 5 minutes, close for 5 minutes and chart the closed-period mean as the ICP; others use a more sophisticated dual-tubing system. Specify your unit's protocol on every handover.
4. The ICP waveform: anatomy of a single cardiac cycle
A clean ICP trace has three readable peaks per cardiac cycle:
- P1, the percussion wave, transmitted directly from the arterial systole via the choroid plexus and large basal arteries. Sharp leading edge. In a healthy compliant brain, P1 is the tallest of the three.
- P2, the tidal wave, a reverberation through the brain parenchyma. Its height tracks compliance: low-compliance brain dampens the parenchymal recoil and P2 grows. P2 > P1 is the hallmark of exhausted compliance.
- P3, the dicrotic wave, following the aortic valve closure transmission. P3 is the smallest in normal compliance; it can merge with P2 as morphology deteriorates.
The amplitude (AMP) is the peak-to-trough of the cardiac pulse, usually 1–4 mmHg in healthy compliance, rising to 6–10 mmHg as compliance falls.
RAP, the compensatory reserve index, is the moving correlation between AMP and mean ICP over a 4-minute window:
- RAP ≈ 0: good compensatory reserve (changes in volume produce little change in pressure, so AMP and mean ICP are uncorrelated).
- RAP → +1: compensatory reserve exhausted (every volume change moves both AMP and mean ICP together).
- RAP falling toward 0 or negative at high ICP: the Marmarou curve has crested; further volume increase brings pressure-volume decompensation. This is a sinister change.
EDV, AMP, and RAP rise before mean ICP. The waveform tells you compensation is failing hours before the mean number breaks through threshold. Train the bedside team to read morphology, not just digits.
5. The numbers to record (the six-pack)
For every patient, on every nursing shift, record this six-pack and trend over time:
| Variable | Symbol | What it tells you |
|---|---|---|
| Mean intracranial pressure | ICP | Bedside threshold for tiered escalation |
| Pulse amplitude | AMP | Compliance state (rises as compliance falls) |
| Compensatory reserve index | RAP | Where on the Marmarou curve we are |
| Cerebral perfusion pressure | CPP = MAP − ICP | Driving pressure to the cortex |
| Pressure reactivity index | PRx | Autoregulatory state (see PRx page) |
| Dose (time x amount above threshold) | ICP-dose, mmHg·h | The outcome-mapped metric |
The dose is the single most important addition to the chart over the past decade. ICP minutes spent above threshold correlate with neurological outcome at 6 months in adult and pediatric severe TBI more tightly than peak ICP or mean ICP. The KidsBrainIT pediatric dataset showed a clear dose-response curve: cumulative ICP > 20 mmHg burden over the first 72 hours predicted GOS-E 6 months later, with a knee at ~8 mmHg·hours below which outcome was unchanged.
This is why bedside teams should think in area under the curve, not point measurements. A patient who spent 6 hours at 25 mmHg has a worse forecast than one who spiked to 35 mmHg for 10 minutes and resolved.
Treat the dose, not the peak. A short spike that resolves to baseline is rarely the issue; a sustained 25 mmHg for hours is. Chart ICP-dose (mmHg·h above threshold) every shift and use it for escalation decisions.
6. What is normal? Age-banded reference values
| Age | Resting ICP (mmHg) | CPP target (mmHg) |
|---|---|---|
| Term newborn (< 28 d) | < 6 | 35–40 |
| Infant 1–11 mo | < 8 | 40–50 |
| Toddler 1–3 y | < 10 | 45–55 |
| Child 4–11 y | < 12 | 50–60 |
| Adolescent 12–18 y | < 15 | 60–70 |
| Healthy adult reference | 7–15 | 60–70 |
Sources: . The guideline target is ICP below 20 mmHg across all ages (treat above 20; Kochanek 2019, PBTF, Level III); there are no separate age-stratified ICP treatment thresholds. Emerging paediatric evidence points lower: sustained ICP above approximately 14 to 15 mmHg is associated with worse outcome, and the field is moving toward ICP dose (intensity x duration) rather than a single cutoff. Pair the number with clinical exam, fontanelle palpation, ONSD, and trend. CPP, by contrast, IS guideline-age-banded (Level III): an individualised CPP target that rises with age, infants at the lower end and adolescents at or above the upper end (see the CPP column above). The neonate column has the weakest evidence base; treat the bedside picture and the fontanelle as much as the number.
Why the pediatric numbers shift with age. Pediatric cerebral autoregulatory range is narrower and shifted left: the lower limit of autoregulation in a toddler may be MAP 45, where in adults it is MAP 60. So a young child tolerates a lower CPP, and pushing CPP toward adult targets can over-perfuse. Resting ICP also reads lower in infants: open fontanelles accommodate volume, so a baseline of 4 to 6 mmHg is normal, not abnormal, in neonates.
7. What is abnormal? A pattern library
| Pattern | Bedside meaning | What to do |
|---|---|---|
| Normal P1 > P2 > P3 | Compliance preserved | Continue monitoring |
| P1 ≈ P2 (marginal) | Reduced compliance | Optimise basics (HOB, sedation, CO2, temperature) |
| Rounded P2 > P1 | Exhausted compliance | Tier 1 + 2 escalation regardless of mean ICP |
| Lundberg A (plateau wave) | 50–100 mmHg above baseline, 5–20 min, then drops | Emergency: hyperosmolar, sedation, head up, consider intervention |
| Lundberg B | 0.5–2 per minute oscillations, 20–40 mmHg | Less specific; investigate sleep, ventilation, sedation depth |
| Lundberg C | 4–8 per minute, low amplitude | Uncertain significance; rarely actionable |
| Sustained ICP > 25 | Mean elevation persistent > 5 min | Tier-based escalation (see Section 8) |
| Rising AMP without mean rise | Compliance loss preceding decompensation | Optimise basics; pre-emptive hyperosmolar consideration |
| Loss of waveform pulsatility | Catheter blocked, kinked, or extreme ICP near cessation | Flush EVD per protocol; check transducer; consider catheter exchange |
Lundberg taxonomy comes from the original 1960 continuous-monitoring monograph that established the modern bedside language. Plateau waves are pathognomonic of low compliance; their amplitude can briefly exceed the operating MAP, producing a brief CPP crash and risk of herniation.
A plateau wave is not just a number; it is an event. Time-stamp it, note the trigger (suctioning, agitation, position change), and act on it. Repeated plateaus mean compliance is critical and pre-emptive escalation is justified even between waves.
8. Try it: interactive widgets
9. ICP-guided CPP management and tiered escalation
This is where the ICP number enters the therapeutic cascade. The pediatric severe-TBI playbook (PBTF 4th edition) organises interventions into three tiers, with thresholds for escalation that depend on time spent above ICP threshold, not on a single peak.
9.1 The CPP target by age (operational)
| Age | Suggested CPP floor (mmHg) | Rationale |
|---|---|---|
| Neonate < 28 d | 35–40 | Narrow autoregulatory band, low baseline MAP |
| Infant 1–11 mo | 40–50 | LLA estimated at MAP ~40 in immature autoregulation |
| Toddler 1–3 y | 45–55 | Transitional; widening LLA |
| Child 4–11 y | 50–60 | Adult-like autoregulatory bandwidth emerging |
| Adolescent 12–18 y | 60–70 | Adult thresholds apply |
CPPopt by PRx is preferred where available (see PRx page and CPPopt page). The age-banded floor is a default; if a PRx-derived U-curve gives a CPPopt of 52 in a 9-year-old, target ±5 mmHg of that, not the table value.
9.2 The tiered escalation pathway
flowchart TD
Read[ICP reading] --> Trend{Mean > threshold<br/>for > 5 min<br/>or rising AMP?}
Trend -->|No| Continue[Continue monitoring]
Trend -->|Yes| Tier1[Tier 1: head up 30 deg,<br/>sedation analgesia,<br/>CSF drainage if EVD,<br/>normocapnia 35-40,<br/>normothermia]
Tier1 --> Persist1{Persists > 20 min?}
Persist1 -->|No| Wean[Continue and reassess]
Persist1 -->|Yes| Tier2[Tier 2: hyperosmolar<br/>3% NaCl 3 mL/kg<br/>or mannitol 0.5 g/kg,<br/>neuromuscular blockade,<br/>repeat CSF drainage]
Tier2 --> Persist2{Persists?}
Persist2 -->|No| Stabilize[Stabilise + reassess]
Persist2 -->|Yes| Tier3[Tier 3: hyperventilation<br/>PaCO2 30-35,<br/>barbiturate coma,<br/>decompressive craniectomy,<br/>mild therapeutic hypothermia]
Tier 1 is the bedside hygiene every PICU should reflexively apply when ICP creeps. Head-of-bed at 30 degrees, neutral midline neck position, optimised sedation and analgesia, normocapnia at PaCO2 35–40, normothermia, sodium 145–155, glucose normal, seizure prophylaxis if EEG suggests need.
Tier 2 introduces hyperosmolar therapy and neuromuscular blockade. Hypertonic saline (3% NaCl bolus 3–5 mL/kg, then infusion to keep sodium 150–155) is generally preferred over mannitol in pediatrics because of stable haemodynamics and the ability to continue infusion. Mannitol 0.25–1 g/kg works as a bolus but carries diuresis and rebound risks.
Tier 3 is the rescue tier. Mild hyperventilation (PaCO2 30–35) reduces CBF acutely and lowers ICP transiently; below 30 it risks ischaemia. Barbiturate coma (pentobarbital infusion to burst suppression on EEG) reduces CMRO2 and ICP but carries refractory hypotension and immune suppression. Decompressive craniectomy is the most definitive intervention; RESCUEicp (adults) and emerging pediatric data show ICP reduction at the cost of unfavourable functional outcomes in survivors.
Decision support, not a clinical protocol. Every threshold and escalation step above is age-, centre-, and patient-dependent. Defer to your unit's protocols and senior clinical team.
10. Clinical contexts: ICP across acute brain injuries
10.1 Severe pediatric TBI
The canonical indication. PBTF 4th-edition guidelines recommend invasive ICP monitoring for children with GCS ≤ 8 and an abnormal CT, individualised CPP target by age, and tiered therapy keyed to ICP > 20 mmHg (all ages). The KidsBrainIT cohort demonstrated the cumulative ICP-dose to outcome relationship that underpins modern "minutes above threshold" thinking.
The BEST-TRIP trial (adults, Bolivia/Ecuador) showed that protocolised ICP-guided care was not superior to imaging/exam-guided care for 6-month outcome. Critics argue the trial recruited a population where ICP monitoring was already not routine and that the result reflects context, not modality. SYNAPSE-ICU observational data (37,000 patients) showed ICP monitoring associated with lower 6-month mortality. The bedside consensus remains: monitor when you can; act on dose, not peak.
10.2 Aneurysmal SAH and IVH
ICP via EVD is the standard placement in aneurysmal SAH with IVH or hydrocephalus, because CSF drainage is itself therapeutic. Adult AHA/ASA 2023 SAH guidelines recommend EVD for symptomatic hydrocephalus and continuous ICP monitoring in poor-grade SAH. Pediatric SAH (often AVM- or trauma-related) follows similar principles but is anatomically different (younger vessels, different aneurysm patterns).
In SAH, rising ICP must be distinguished from vasospasm-driven flow changes: ICP can be stable while TCD MFV rises (vasospasm without ICP rise) or rising independently (rebleed, acute hydrocephalus, oedema). This is the canonical "pair ICP with TCD" scenario.
10.3 HIE and post-cardiac arrest
Routine ICP monitoring in HIE / post-arrest is not standard. The Eurotherm-3235 and THAPCA cohorts did not use invasive ICP. Selective use in patients with malignant cerebral oedema documented on imaging is centre-dependent. Non-invasive surrogates (ONSD, NIRS, fontanelle US in infants) are the more common bedside tools.
10.4 Bacterial meningitis with raised ICP
Pediatric bacterial meningitis can produce both communicating hydrocephalus (from inflammatory blockade of CSF absorption) and cerebral oedema. EVD placement is the first-line invasive monitor when raised ICP is documented or strongly suspected. The European meningitis guidelines and IDSA encephalitis guidelines acknowledge ICP monitoring as a tier-2 intervention in severe cases.
10.5 Hydrocephalus and shunt malfunction
ICP monitoring is used both diagnostically (overnight ICP recordings in suspected shunt failure, looking for B waves) and therapeutically (EVD as bridging in acute shunt failure pre-revision). The ESPVS style of overnight ICP-trend recording remains a useful diagnostic for shunt under-drainage.
10.6 DKA cerebral oedema
A pediatric-specific case where ICP monitoring is rarely invasive in time. Cerebral oedema in DKA classically presents 4–12 hours into rehydration, with rapid clinical deterioration (headache, altered consciousness, then herniation). The PECARN FLUID trial showed that fluid-rate choice did not change cerebral-oedema rates; the bedside priority is early recognition with neurological scoring, hypertonic saline 3% bolus, and CT, rather than waiting for an invasive monitor. ONSD and clinical scoring are the practical bedside tools.
10.7 Hepatic encephalopathy with cerebral oedema
Acute liver failure can produce ammonia-driven cerebral oedema that is the most common cause of death in fulminant hepatic failure. Invasive ICP monitoring is contentious because of the bleed risk from coagulopathy; transfused factor support before placement reduces but does not eliminate this. Many centres now favour non-invasive monitoring (ONSD, jugular bulb saturation, EEG) until coagulation supports a safer invasive placement.
10.8 Post-stroke malignant MCA and decompressive craniectomy
Large-vessel ischaemic stroke with malignant oedema is a pediatric emergency in older children. Decompressive hemicraniectomy within 48 hours of clinical decline improves survival but at the cost of disability; ICP monitoring post-decompression is sometimes used to titrate medical therapy through the swelling phase.
11. Multimodal integration: ICP in the MMM/MNM stack
ICP is the bedrock invasive number, but alone it answers only one question. Pair with the modalities below to answer the others.
| Pair with… | What you gain | Worked scenario |
|---|---|---|
| PRx | Autoregulatory state and CPPopt derivation | PRx page, CPPopt page |
| TCD | Spasm vs rising-ICP discrimination; non-invasive ICP backup via PI; Mx autoregulation | TCD vs ICP vasospasm |
| NIRS | Tissue oxygenation surrogate when ICP is normal but tissue is suffering; non-invasive backup when ICP cannot be placed | PRx vs COx discordance |
| PbtO2 | Tissue oxygenation gold-standard pair (the BOOST triplet: ICP + PbtO2 + PRx) | PbtO2-CPP titration |
| EEG / cEEG | Seizure-driven ICP elevations (NCSE causes both ICP spikes and metabolic demand) | EEG / TCD pair |
| Pupillometry (NPi) | Brainstem function and herniation early warning | NPi page |
| ONSD | Non-invasive ICP cross-check at bedside (especially when EVD is unreliable) | ONSD page |
| Microdialysis | Metabolic crisis (lactate/pyruvate ratio) at ICP "acceptable" levels | Microdialysis page |
| Clinical exam | Most important pairing; an isolated ICP number is dangerous | Always |
12. Setup and technique: a step-by-step
12.1 Site selection
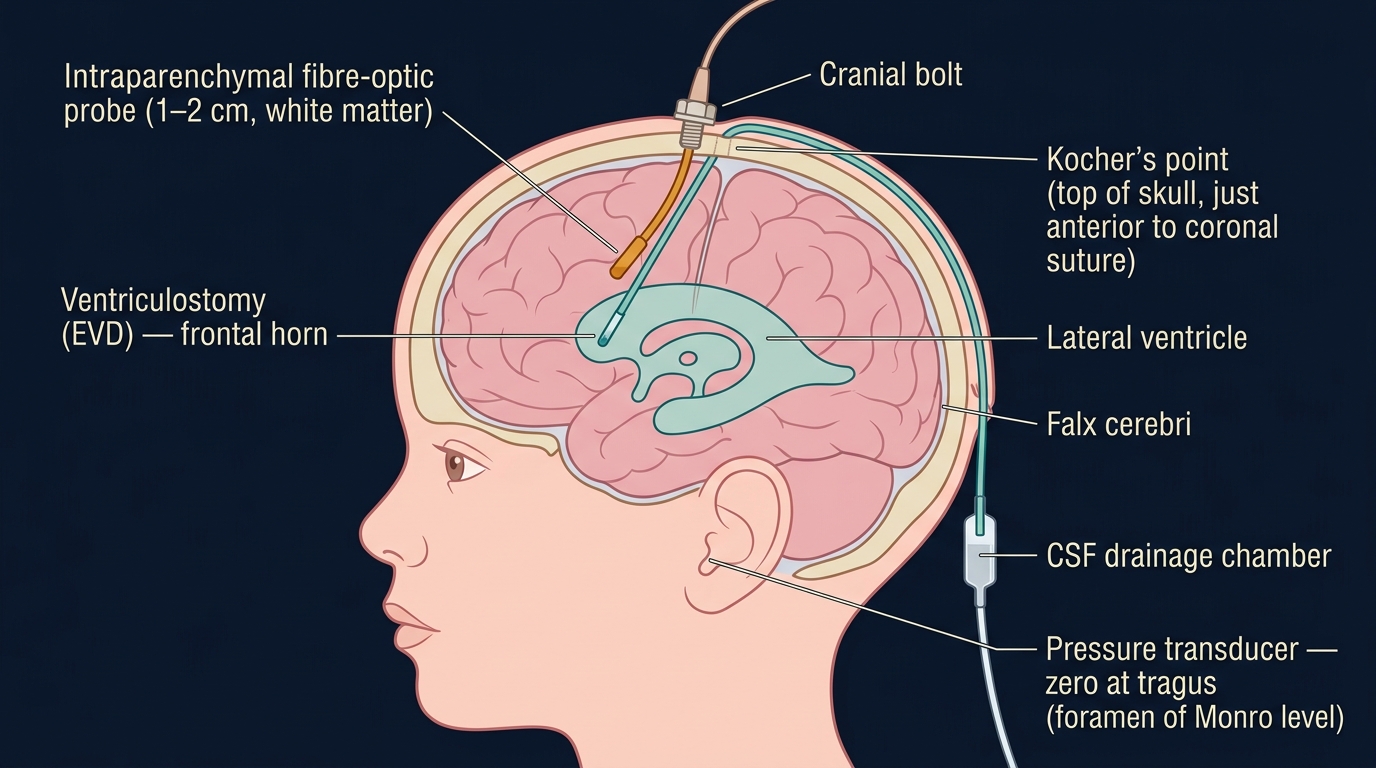
Kocher's point is the canonical entry: ~2.5 cm lateral to the sagittal midline at the coronal suture (or ~10 cm posterior to the nasion, ~2.5 cm lateral), on the non-dominant hemisphere (right-sided in most). This avoids the motor strip and the sagittal sinus, and the trajectory through frontal white matter has the least eloquent cortex.
Frazier's point (~6 cm above and 3 cm lateral to the inion) targets the occipital horn for posterior approaches.
12.2 Intraparenchymal probe insertion
- Position head neutral, skin shaved over the entry site, sterile prep and drape.
- Local anaesthetic (lidocaine + adrenaline subcutaneously).
- Skin incision 5–10 mm vertical stab.
- Burr hole with twist drill or hand-cranked perforator.
- Dural puncture through the bolt with a small spinal needle.
- Probe self-zeroing in air (intraparenchymal probes calibrate once, pre-insertion, then never again).
- Insertion to fixed depth (typically 1–2 cm into white matter).
- Bolt locked to skull.
- Display: connect to monitor, confirm three-peak waveform with respiratory swing and cardiac pulse, document baseline ICP and morphology.
12.3 EVD insertion
Same approach through burr hole, then a silicone catheter is passed ~5–7 cm to enter the frontal horn of the lateral ventricle. CSF egress confirms placement. The catheter is fluid-coupled through saline-filled tubing to an external pressure transducer.
12.4 Zeroing, the most-missed source of error
- Fluid-coupled (EVD): zero the transducer to atmosphere at tragus level (corresponds to foramen of Monro at supine). If the transducer drifts up or down with the patient's head position, ICP changes by ~7 mmHg per 10 cm. Re-zero every shift and after every position change.
- Intraparenchymal: self-zero before insertion, never again. Drift over days (typically 1–3 mmHg by day 5) is the trade-off.
12.5 Signal quality cues
- Clean three-peak waveform with P1 > P2 > P3 in normal compliance: trust.
- Respiratory swing of 1–4 mmHg: confirms patency.
- Cardiac pulse present: confirms vascular coupling.
- No swing, no pulse, dead-line trace: catheter is blocked, kinked, or the transducer is disconnected. Flush per local protocol; do not act on a flat-line ICP.
12.6 Infection prevention
Bundle elements with the strongest evidence: chlorhexidine prep, full-barrier draping, antibiotic-impregnated catheters (silver-coated or rifampicin/minocycline-impregnated), tunnelled subcutaneous track ≥ 5 cm, closed drainage system with no breaks, no routine prophylactic systemic antibiotics. Infection rate climbs from ~2% in week 1 to ~10% by week 2. Plan exchange or removal at day 5–7 if still needed and clinical state allows.
12.7 EVD drain management
The two competing modes:
- Continuous drainage with set level: drain set at 10–20 cm H2O above tragus; CSF drains continuously when ICP exceeds that. ICP is not readable while draining.
- Intermittent drainage with monitoring: drain closed for monitoring, opened for 5-minute intervals when ICP exceeds threshold or per shift schedule. ICP is readable during closed periods.
Most centres now favour intermittent monitoring with set-level drainage to allow ICP measurement and CPP calculation; trial data is mixed and unit protocols vary widely.
13. Pitfalls and artefacts
- Drift in fibre-optic probes (typically < 3 mmHg/day, but cumulative over a week).
- Damping of fluid-coupled EVDs from bubbles, kinks, or clots; characteristic loss of waveform pulsatility.
- Open EVD continuously zeroes ICP to the drainage chamber height; cannot read true ICP through an open drain.
- Transducer height changes: every 10 cm above tragus reads ICP ~7 mmHg too low; every 10 cm below reads it ~7 mmHg too high.
- Coughing, suctioning, bucking: transient ICP spikes via thoracic pressure transmission. Note in trace; do not act unless sustained or recurrent.
- Sedation effects on baseline: deep propofol reduces CMRO2 and lowers baseline ICP by ~3–5 mmHg; lightening sedation should prompt a re-baseline.
- Compartmentalised oedema (e.g., temporal lobe contusion behind a closed tentorium): regional pressure can be much higher than the supratentorial probe reads. ICP can be "normal" while the pupil blows.
- Slit ventricles: EVD placement fails ~5% from inability to cannulate; use intraparenchymal instead.
- Sodium driving ICP: hyponatremia (< 130) raises ICP via brain oedema; correct cautiously to avoid osmotic demyelination.
- PEEP transmission: PEEP > 10–12 transmits to ICP via venous outflow resistance, especially with reduced lung compliance. See PEEP-ICP-MAP demo.
14. Combine with…
- CPP: driving pressure = MAP − ICP, the partner to every ICP measurement.
- PRx: autoregulatory state through this very ICP signal.
- CPPopt: individualised target derived from the PRx-CPP relationship.
- RAP: what the ICP waveform tells you about compliance.
- Non-invasive ICP: when invasive placement is contraindicated or unavailable.
- ONSD: bedside ultrasound surrogate.
- TCD: flow consequence of the same physiology and a spasm-vs-ICP discriminator.
- PbtO2: tissue oxygenation pair (the BOOST triplet).
- Pupillometry: brainstem early warning.
15. Evidence summary and recent literature
15.1 Evidence summary
| Topic | Source | Grade |
|---|---|---|
| Monro-Kellie doctrine | foundational | |
| Marmarou pressure-volume relationship | A (foundational) | |
| Lundberg waves taxonomy | foundational | |
| ICP pulse waveform analysis | B | |
| ICP-targeted therapy in severe TBI (peds) | B | |
| BEST-TRIP, ICP-targeted vs exam-targeted (adults) | A | |
| SYNAPSE-ICU, ICP monitoring and mortality | B | |
| Decompressive craniectomy (RESCUEicp, DECRA) | A | |
| ICP dose-response to outcome (KidsBrainIT) | B | |
| Pediatric MNM consensus | expert | |
| Neurocritical Care Society MMM consensus | expert | |
| ICP best practice consensus 2014 | expert | |
| CPPopt by PRx | B | |
| Pediatric CPPopt | B |
15.2 Recent literature (2022–2025)
- COGiTATE phase II (Beqiri 2024): adult severe TBI trial demonstrating CPPopt-guided care is feasible and safe, with secondary endpoints suggesting outcome benefit. The pediatric extension is awaited but Tas 2024 single-centre data already supports the concept in children.
- Pediatric MNM consensus 2025 (Figaji): formalises ICP as the anchor invasive modality and stratifies tier-2 modalities (PbtO2, microdialysis, PRx-derived CPPopt) by resource level.
- Non-invasive ICP estimators: Brain4Care-style waveform-derived nICP (Brasil 2021, 2022; Cardim 2023; Rasulo 2024). Useful for triage and trend-following but not a replacement for invasive measurement in patients with established intracranial hypertension.
- ICP dose vs outcome (Guiza 2015 + follow-on): the cumulative-dose framework is now the standard outcome-mapped metric and is increasingly built into ICU-grade ICP monitoring systems.
- SYNAPSE-ICU follow-on: ICU-level variability in ICP monitoring practice remains substantial; calls for international standardisation of indications and thresholds.
16. Self-check
References
- Kochanek PM, Tasker RC, Carney N, et al.. Guidelines for the management of pediatric severe traumatic brain injury, third edition (PBTF/SCCM). Pediatric Critical Care Medicine 2019;20(3S):S1-S82.
- Hutchinson PJ, Kolias AG, Timofeev IS, et al.. Trial of decompressive craniectomy for traumatic intracranial hypertension. New England Journal of Medicine 2016;375(12):1119–1130. doi:10.1056/NEJMoa1605215 link
- Kazimierska A, Kasprowicz M, Czosnyka M, et al.. Compliance of the cerebrospinal space: comparison of three methods. Acta Neurochirurgica 2021;163(7):1979–1989. doi:10.1007/s00701-021-04834-y link
- Padayachy LC, Padayachy V, Galal U, Pollock T, Fieggen AG. The relationship between transorbital ultrasound measurement of the optic nerve sheath diameter and invasive ICP in children. Part I: repeatability, observer variability and general analysis. Childs Nervous System 2016;32(10):1769-1778.
- Cardim D, Robba C, Bohdanowicz M, et al.. Non-invasive monitoring of intracranial pressure using transcranial Doppler ultrasonography: is it possible?. Neurocritical Care 2016;25:473-491.
- Hoh BL, Ko NU, Amin-Hanjani S, et al.. Guideline for the management of patients with aneurysmal subarachnoid hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke 2023;54(7):e314-e370.
- Rass V, Helbok R. How to diagnose delayed cerebral ischaemia and symptomatic vasospasm and prevent cerebral infarction in patients with subarachnoid haemorrhage. Current Opinion in Critical Care 2021;27(2):103-114.
- Marmarou A, Shulman K, Rosende RM. A nonlinear analysis of the cerebrospinal fluid system and intracranial pressure dynamics. Journal of Neurosurgery 1978;48(3):332–344. doi:10.3171/jns.1978.48.3.0332 link
- Avezaat CJJ, van Eijndhoven JHM, Wyper DJ. Cerebrospinal fluid pulse pressure and intracranial volume-pressure relationships. Journal of Neurology, Neurosurgery, and Psychiatry 1979;42(8):687–700. doi:10.1136/jnnp.42.8.687 link
- Czosnyka M, Pickard JD. Monitoring and interpretation of intracranial pressure. Journal of Neurology, Neurosurgery, and Psychiatry 2004;75(6):813–821. doi:10.1136/jnnp.2003.033126 link
- Tasker RC. Cerebrovascular reactivity in pediatric severe traumatic brain injury: a review. Pediatric Critical Care Medicine 2023.
- Chesnut RM, Temkin N, Carney N, et al.. A trial of intracranial-pressure monitoring in traumatic brain injury. NEJM 2012;367(26):2471-2481.
- Hawthorne C, Piper I. Monitoring of intracranial pressure in patients with traumatic brain injury. Frontiers in Neurology 2014;5:121.
- Czosnyka M, Guazzo E, Whitehouse M, et al.. Significance of intracranial pressure waveform analysis after head injury. Acta Neurochirurgica 1996;138(5):531–541. doi:10.1007/BF01411173 link
- Kim DJ, Carrera E, Czosnyka M, Keong N, Smielewski P, Pickard JD. Index of cerebrospinal compensatory reserve in hydrocephalus. Neurosurgery 2009;64(3):494–501.
- Guiza F, Depreitere B, Piper I, et al.. Visualizing the pressure and time burden of intracranial hypertension in adult and paediatric TBI. Intensive Care Medicine 2015;41(6):1067-1076.
- Depreitere B, Guiza F, Van den Berghe G, et al.. Pressure autoregulation monitoring and CPP target recommendation in patients with severe TBI based on minute-by-minute monitoring data. Journal of Neurosurgery 2014;120(6):1451-1457.
- Tasker RC, Lewis PM, White DK, Smith CA, Hutchinson PJ, Lyons RA. Pediatric multimodal monitoring: clinical and research priorities. Pediatric Critical Care Medicine 2023.
- Agrawal S, Bögli SY, O'Donnell R, et al.. Intracranial Pressure Treatment Thresholds in Pediatric Traumatic Brain Injury. JAMA Pediatrics 2026;180(6):650-658. doi:10.1001/jamapediatrics.2026.0197 link
- Svedung Wettervik T, Velle F, Hånell A, et al.. ICP, PRx, CPP, and ΔCPPopt in pediatric traumatic brain injury: the combined effect of insult intensity and duration on outcome. Child's Nervous System 2023;39(9):2459-2466. doi:10.1007/s00381-023-05982-5 link
- Brady KM, Mytar JO, Lee JK, et al.. Monitoring cerebral blood flow pressure autoregulation in pediatric patients during cardiac surgery. Stroke 2010;41(9):1957–1962. doi:10.1161/STROKEAHA.109.575167 link
- Lundberg N. Continuous recording and control of ventricular fluid pressure in neurosurgical practice. Acta Psychiatrica et Neurologica Scandinavica 1960;36(Suppl 149):1–193.
- Aries MJ, Czosnyka M, Budohoski KP, et al.. Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury. Critical Care Medicine 2012;40(8):2456-2463.
- Beqiri E, Smielewski P, Robba C, Czosnyka M, et al.. Feasibility of individualised severe TBI management using a CPPopt approach: COGiTATE phase II trial. Intensive Care Medicine 2021;47:1093-1103.
- Tas J, Beqiri E, van Kaam C, et al.. An update on the COGiTATE Phase II study: feasibility and safety of targeting CPPopt in adult TBI patients. Acta Neurochir Suppl 2022.
- Tas J, Smielewski P, Aries MJ, Czosnyka M, Tasker RC. Feasibility of pediatric CPPopt monitoring in severe TBI. Frontiers in Pediatrics 2024.
- Cottenceau V, Masson F, Mahamid E, et al.. Comparison of effects of equiosmolar doses of mannitol and hypertonic saline on cerebral blood flow and metabolism in traumatic brain injury. Journal of Neurotrauma 2011;28(10):2003–2012. doi:10.1089/neu.2011.1929 link
- Cooper DJ, Rosenfeld JV, Murray L, et al.. Decompressive craniectomy in diffuse traumatic brain injury. New England Journal of Medicine 2011;364(16):1493–1502. doi:10.1056/NEJMoa1102077 link
- Robba C, Graziano F, Rebora P, et al.. Intracranial pressure monitoring in patients with acute brain injury in the intensive care unit (SYNAPSE-ICU): an international, prospective observational cohort study. Lancet Neurology 2021;20(7):548–558. doi:10.1016/S1474-4422(21)00138-1 link
- Shankaran S, Laptook AR, Ehrenkranz RA, et al.. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. NEJM 2005;353(15):1574-1584.
- Moler FW, Silverstein FS, Holubkov R, et al.. Therapeutic hypothermia after out-of-hospital cardiac arrest in children (THAPCA-OH). NEJM 2015;372(20):1898-1908.
- Naim MY, Friess SH, Sutton RM, et al.. Multimodal neuromonitoring in pediatric post-cardiac-arrest care. Pediatric Critical Care Medicine 2023.
- van de Beek D, Cabellos C, Dzupova O, et al.. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clinical Microbiology and Infection 2016;22 Suppl 3:S37-S62.
- Tunkel AR, Glaser CA, Bloch KC, et al.. The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. Clinical Infectious Diseases 2008;47(3):303-327.
- Tunkel AR, Hartman BJ, Kaplan SL, et al.. Practice guidelines for the management of bacterial meningitis (IDSA). Clinical Infectious Diseases 2004;39(9):1267–1284.
- Eide PK. A new method for processing of continuous intracranial pressure signals. Medical Engineering & Physics 2006;28(6):579–587. doi:10.1016/j.medengphy.2005.09.008 link
- Kuppermann N, Ghetti S, Schunk JE, et al.. Clinical trial of fluid infusion rates for pediatric diabetic ketoacidosis (PECARN FLUID). NEJM 2018;378(24):2275-2287.
- Glaser N, Kuppermann N. Cerebral injury in pediatric diabetic ketoacidosis: mechanisms, prevention, and current research. Pediatric Diabetes 2024.
- Glaser N, Barnett P, McCaslin I, et al.. Risk factors for cerebral edema in children with diabetic ketoacidosis. NEJM 2001;344(4):264–269.
- Muir AB, Quisling RG, Yang MCK, Rosenbloom AL. Cerebral edema in childhood diabetic ketoacidosis: natural history, radiographic findings, and early identification. Diabetes Care 2004;27(7):1541–1546.
- Vespa PM, Boscardin WJ, Hovda DA, et al.. Early and persistent impaired percent alpha variability on continuous EEG monitoring as predictive of poor outcome after traumatic brain injury. Journal of Neurosurgery 2002;97(1):84–92. doi:10.3171/jns.2002.97.1.0084 link
- Ferriero DM, Fullerton HJ, Bernard TJ, et al.. Management of stroke in neonates and children: a scientific statement from the AHA/ASA. Stroke 2019;50(3):e51-e96.
- Sun LR, Wilson JL, Waak M, et al.. Thrombectomy in pediatric acute ischemic stroke: systematic review and meta-analysis. Pediatric Neurology 2020;105:11-19.
- Figaji AA, Tasker RC, Bell MJ, Kochanek PM. Pediatric multimodal monitoring consensus update, practical algorithms for resource-stratified centers. Intensive Care Medicine, Paediatric and Neonatal 2025.
- Helbok R, Tasker RC, Kochanek PM, Bell MJ. Pediatric multimodal monitoring: where are we and where do we go?. Pediatric Critical Care Medicine 2024.
- Le Roux P, Menon DK, Citerio G, et al.. Consensus summary statement of the international multidisciplinary consensus conference on multimodality monitoring in neurocritical care. Intensive Care Medicine 2014;40(9):1189-1209.
- Monro A. Observations on the structure and functions of the nervous system. Edinburgh: Creech & Johnson 1783.
- Kellie G. An account of the appearances observed in the dissection of two of the three individuals presumed to have perished in the storm of the 3rd, and whose bodies were discovered in the vicinity of Leith on the morning of the 4th of November 1821. Transactions of the Medico-Chirurgical Society of Edinburgh 1824;1:84–169.
- Mokri B. The Monro-Kellie hypothesis: applications in CSF volume depletion. Neurology 2001;56(12):1746–1748. doi:10.1212/wnl.56.12.1746 link
- Tasker RC, LaRovere KL, Riviello JJ, et al.. Pediatric multimodal neuromonitoring: international Delphi consensus. Pediatric Critical Care Medicine 2023.
- Tas J, Beqiri E, Czosnyka M, Aries MJ, Smielewski P. COGiTATE follow-up: long-term outcomes of CPPopt-targeted management in adult TBI. Journal of Neurotrauma 2025.
- Brasil S, Solla DJF, Nogueira RC, Teixeira MJ, Malbouisson LMS, Paiva WS. A novel non-invasive technique for intracranial pressure waveform monitoring in critical care. Journal of Personalized Medicine 2021;11(12):1302. doi:10.3390/jpm11121302 link
- Brasil S, Solla DJF, Nogueira RC, Teixeira MJ, Malbouisson LMS, Paiva WS. Intracranial compliance and cerebral perfusion: novel non-invasive assessment using waveform analysis. Brain Sciences 2022;12(11):1559.
- Cardim D, Robba C, Czosnyka M, et al.. Non-invasive ICP estimation: an updated review. J Clin Monit Comput 2023.
- Rasulo FA, Brasil S, Andrade R, Robba C. Non-invasive ICP estimation by Brain4Care: prospective validation across centers. Neurocritical Care 2024.