Transcranial Doppler / TCCD
A 2 MHz probe through the temporal window, and a window onto cerebral hemodynamics, vasospasm, raised ICP, autoregulation, and CPP titration. Pediatric-first.
1. Bedside vignettes: why this matters in the PICU
Vignette A. Pediatric SAH day 6, suspected vasospasm
A 12-year-old presents with a ruptured AVM and aneurysmal SAH. On day 6 the nurse notices a subtle right-arm drift. You bring the TCD cart, slide the probe over the right temporal window, and within seconds the familiar saw-tooth velocity envelope appears. PSV 220, EDV 90, MFV 130, PI 1.0. The team checks the extracranial ICA: MFV 30. Lindegaard ratio 4.3, mild-to-moderate vasospasm. You alert neurosurgery, escalate haemodynamics, and schedule angiography.
Vignette B. Severe TBI, the ventriculostomy is delayed
A 4-year-old fell from a roof. GCS 6, blown pupil on the right, CT shows a large temporal contusion with effacement of the basal cisterns. Theatre is 30 minutes away and a parenchymal monitor is not on the unit. You scan the left MCA: MFV 28, EDV 7, PI 1.8. The diastolic notch is shallow; the Bellner regression returns ICP ≈ 28 mmHg. You mannitol, raise the head, and call again. By the time the team is in theatre, TCD PI has fallen to 1.2.
Vignette C. Post-arrest HIE, day 2
A newborn cools after a tight nuchal cord and meconium aspiration. Day 2, rewarmed. NIRS rSO₂ has risen to 88%. TCD MCA: PSV 110, EDV 60, PI 0.5, MFV 80. The diastolic shoulder is high and the envelope looks "lush." This is luxury perfusion: relative hyperaemia in a brain whose metabolism has collapsed. A low PI with high EDV in HIE is not reassurance; coupled with isoelectric aEEG it is one of the worst prognostic signatures.
2. What TCD is, and what it is not
TCD is a handheld pulsed-wave ultrasound at ~2 MHz, low enough to penetrate the thin parts of the skull, that measures the velocity of red blood cells in the basal cerebral arteries. The Doppler shift formula is:
where Δf is the frequency shift, f₀ the transmitted frequency, v the blood velocity, θ the angle of insonation, and c the speed of sound in tissue.
Two things follow immediately.
TCD measures velocity, not flow. Flow is velocity × cross-sectional area. The cross-section of the M1-MCA changes with vasospasm, hypocapnia, fever, sedation, and anaesthetic. If a vessel narrows by 50%, velocity must roughly quadruple to preserve flow. So a rise in MFV may mean the same flow through a smaller pipe (vasospasm), or more flow through an unchanged pipe (hyperaemia), or both. The Lindegaard ratio exists to discriminate these.
TCD requires an angle assumption. Blind TCD assumes cos θ ≈ 1 (the operator hand-aims for the loudest signal). TCCD images the vessel in B-mode first, corrects the angle, and is preferred where available, especially in children, where the temporal bone is thin and the vessels are close to the probe.
"Velocity ≠ flow" is the single most important sentence on this page. Every paradoxical TCD reading you will encounter starts there. Repeat it before you interpret any number.
Pediatric skulls are thinner; windows are usually excellent. Insonation depths are also shallower: M1-MCA is at ≈ 30–40 mm in toddlers and ≈ 40–50 mm in school-age children versus 45–55 mm in adults. Adjust the depth gate before searching for the signal or you will be insonating distal branches.
3. The four insonation windows
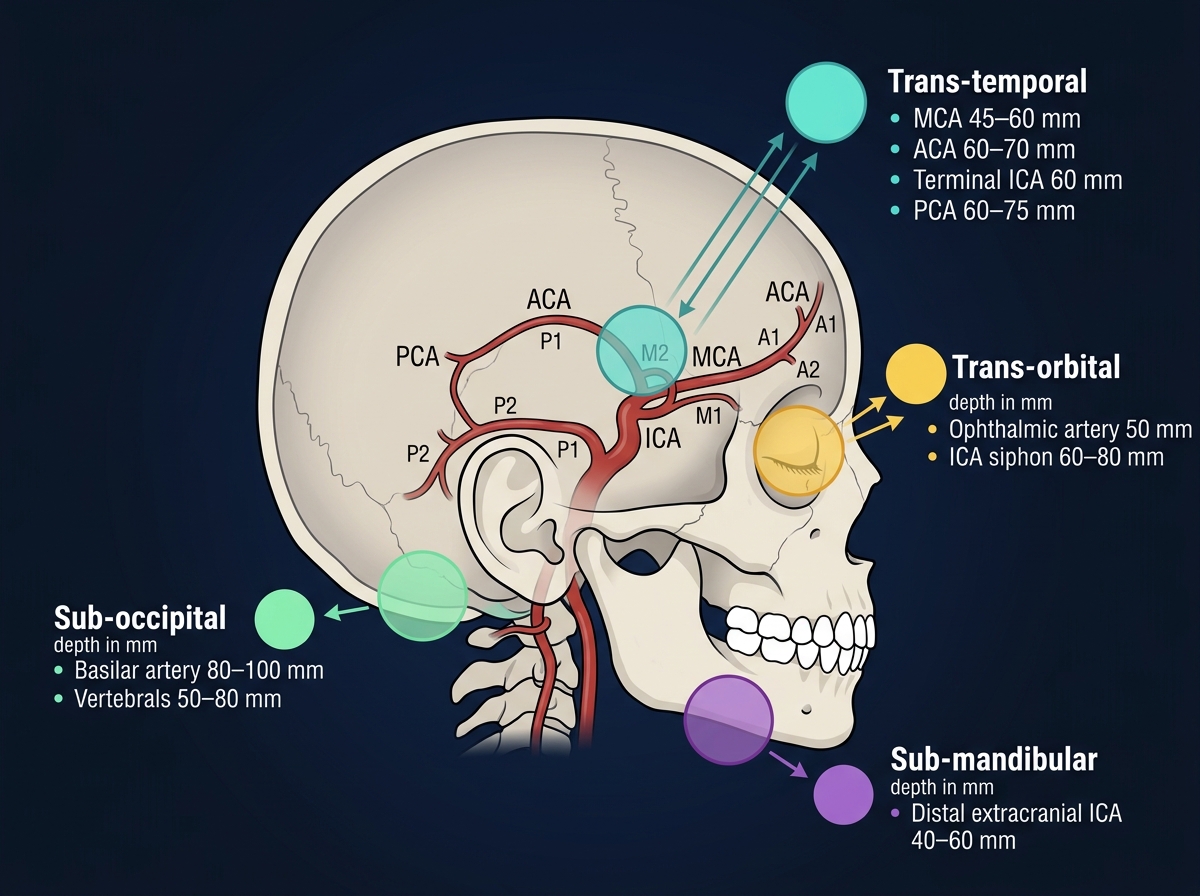
| Window | Vessel | Typical depth | Flow direction (toward / away from probe) |
|---|---|---|---|
| Transtemporal | MCA (M1) | 45–55 mm (adult) / 30–45 mm (child) | Toward |
| Transtemporal | MCA (M2) | 30–40 mm | Toward / bidirectional |
| Transtemporal | ACA (A1) | 60–75 mm | Away |
| Transtemporal | PCA (P1) | 60–75 mm | Toward |
| Transtemporal | TICA | 60–65 mm | Toward |
| Transorbital | Ophthalmic | 40–60 mm | Toward |
| Transorbital | ICA siphon | 60–80 mm | Bidirectional |
| Suboccipital | Vertebrals | 60–75 mm | Away |
| Suboccipital | Basilar | 80–120 mm | Away |
| Submandibular | Extracranial ICA | 50–60 mm | Away |
Always confirm the vessel. Depth alone is not enough; manoeuvres (carotid tap on the neck transiently dampens the MCA envelope; head turn changes vertebral signal) confirm the identity of the artery before you record a number.
4. The spectral waveform: anatomy of a TCD trace
A normal MCA spectral envelope has four readable features.
- A sharp systolic upstroke, driven by the cardiac systole reaching the cerebral circulation, propagated through compliant proximal arteries.
- A clean systolic peak (PSV), the maximum velocity recorded in that cardiac cycle.
- A dicrotic notch, the small inflection between PSV and the diastolic trough; it corresponds to aortic-valve closure. In a very high-resistance circulation (e.g., severe raised ICP) the notch deepens and may disappear into a true reverse-flow trough.
- A diastolic shoulder falling to EDV, the floor of the cardiac cycle. EDV is the most sensitive single number to changes in downstream resistance: it falls when ICP rises, when small-vessel vasoconstriction occurs (hypocapnia), or when distal capacitance is lost.
The mean (MFV) is the time-weighted average of the entire envelope across the cycle. A common bedside approximation, accurate to within ~5%, is:
PI (Gosling) captures the pulsatility, the height of the envelope relative to its mean. RI is similar but normalised to PSV. Both rise when distal resistance rises. PI ~ 0.5–1.1 is the healthy range across most ages. PI > 1.4 is "high"; PI > 2.0 with low or absent EDV is the territory of impending arrest.
EDV is the most informative single number on the trace. A falling EDV with rising PI is the earliest TCD signature of rising ICP, well before MFV starts to fall.
5. The numbers: what to record, in what order
For every patient, on every side, record this six-pack:
| Variable | Symbol | What it tells you |
|---|---|---|
| Peak systolic velocity | PSV | Cardiac output × proximal vessel patency. Use as a screening glance; large absolute changes matter. |
| End-diastolic velocity | EDV | Distal resistance. Falls when ICP rises, when vessels constrict (hypocapnia, hyperoxia), or when capacitance is lost. |
| Mean flow velocity | MFV | The bedside index of cerebral perfusion. Use age-banded reference values in children. |
| Pulsatility index | PI | (PSV − EDV) / MFV. Rises with distal resistance. Most useful single derived number. |
| Lindegaard ratio | LR | MCA MFV ÷ extracranial ICA MFV. Separates vasospasm (LR > 3) from hyperaemia (LR < 3). |
| Time-averaged maximum mean velocity | TAMMV | STOP-trial index for sickle cell disease (≥ 200 cm/s = abnormal). |
Record both sides and look for asymmetry > 30%. Asymmetric MFV is the bedside signature of unilateral vasospasm, embolic occlusion, or unilateral raised ICP from a mass lesion.
6. What is normal? Age-banded reference values
Healthy MCA MFV is highest in early childhood, when cerebral metabolic rate per gram of brain peaks, and falls into adolescence and adulthood.
| Age | MCA MFV (cm/s, mean ± SD) | LLA / ULA bedside heuristic |
|---|---|---|
| Term newborn (< 7 d) | 24 ± 7 | very narrow; assume passive flow below MAP ~ 30 |
| 1–3 months | 42 ± 10 | LLA ≈ MAP 35–40 |
| 6 months | 74 ± 14 | LLA ≈ MAP 40–45 |
| 1–3 years | 85 ± 10 | LLA ≈ MAP 45–55 |
| 4–6 years | 97 ± 9 (peak) | LLA ≈ MAP 50–60 |
| 7–11 years | 89 ± 9 | LLA ≈ MAP 55–65 |
| 12–18 years | 75 ± 13 | LLA ≈ MAP 60–70 |
| Healthy adult | 55 ± 12 | LLA ≈ MAP 60–70, ULA ≈ 150 |
Sources: . LLA / ULA columns are bedside heuristics; autoregulation in children is narrower and lower than the adult Lassen plateau, and the lower limit is dangerously close to baseline MAP in infants.
The pediatric MFV norm in a 5-year-old (~100 cm/s) would suggest moderate vasospasm in an adult. Reading TCD MFV without an age-band reference is the single most common pediatric TCD error. Trend against the child's own baseline and against ratios (LR) before reading absolute values.
7. What is abnormal? A small pattern library
| Pattern | Bedside meaning | What to do |
|---|---|---|
| High MFV + LR > 3 | Vasospasm (not hyperaemia) | Treat; escalate haemodynamics; angiography if clinical signs |
| High MFV + LR < 3 | Hyperaemia / luxury perfusion | Look for cause (fever, sepsis, anaemia, post-hypoxic, hyperaemic phase of TBI) |
| High PI (> 1.4) + normal MFV | Raised intracranial resistance: high ICP, hypocapnia, vasoconstrictors | Recheck etCO₂; consider ICP measurement |
| Low EDV + high PI | Falling cerebral perfusion pressure | Treat aggressively; reassess CPP |
| Oscillating / reverse EDV | Impending circulatory arrest | Confirm and act; call for ancillary brain-death testing if clinically appropriate |
| Reverberating / "pendular" trace | Cerebral circulatory arrest | Document, repeat at 30 min as per local brain-death protocol |
| Systolic spikes only | Pre-arrest pattern | Same as oscillating; confirm and escalate |
| TAMMV ≥ 200 cm/s in SCD | Stroke risk; STOP trigger | Chronic transfusion (STOP protocol) |
| Asymmetric MFV > 30% | Unilateral spasm, occlusion, mass lesion, or window asymmetry | CT / MR if clinically warranted |
Reverse diastolic flow is a near-pathognomonic sign of severely impaired cerebral perfusion or imminent cerebral circulatory arrest. Confirm bilaterally, document, and act.
Decision tree: "what question am I asking?"
flowchart TD
Reading[TCD spectrum] --> Why{What is asked?}
Why -->|SCD stroke screening| TAMV[TAMMV]
TAMV --> SCDtier{Value}
SCDtier -->|< 170| Normal[Normal, annual screen]
SCDtier -->|170–199| Cond[Conditional, repeat sooner]
SCDtier -->|≥ 200| Abn[Abnormal, chronic transfusion per STOP]
Why -->|Vasospasm in SAH| LRcalc[Lindegaard ratio]
LRcalc -->|LR > 3 + high MFV| Spasm[Vasospasm; treat]
LRcalc -->|LR < 3 + high MFV| Hyper[Hyperaemia; look for cause]
Why -->|Raised ICP suspected| PIcheck[PI + EDV]
PIcheck -->|PI > 1.4, low EDV| Resist[Likely high ICP / low CPP]
PIcheck -->|Oscillating EDV| Arrest[Pre-arrest; escalate]
Why -->|Autoregulation| Mxcalc[Mx slow-wave correlation]
Mxcalc -->|Mx < 0.3| Intact[Intact]
Mxcalc -->|Mx > 0.3| Impaired[Impaired; re-target CPP]
8. Try it: interactive widgets
9. TCD-guided blood-pressure and CPP management
This is where TCD earns its place in the multimodal stack. Two TCD-derived indices, Mx (autoregulation index) and CCP (critical closing pressure), let you reason about this patient's upper and lower BP limits without an invasive ICP monitor.
9.1 Can TCD set BP targets on its own?
Short answer: not by itself, but it can narrow the range.
- MFV trend across BP changes: If MFV moves linearly with MAP (passive flow), the patient is outside their autoregulatory plateau: either MAP is too low (below LLA) or too high (above ULA), or autoregulation is broken entirely. If MFV stays flat across MAP swings, autoregulation is intact and current MAP is on the plateau.
- PI as a CPP / ICP proxy: PI rises as CPP falls. The Bellner regression (ICP ≈ 10.93 · PI − 1.28) is the most cited bedside formula, with confidence intervals wide enough that it is a triage tool, not a measurement tool.
- Trend over absolute: A 50% rise in PI from baseline is informative; a single PI of 1.3 is not.
PI is not ICP. PI rises with anything that raises distal cerebrovascular resistance, including hypocapnia, hyperoxia, low arterial compliance (in neonates), and cold extremities (probe coupling artefact). de Riva et al's 2012 review is the canonical "don't do this" paper on PI-as-ICP substitution.
9.2 Mx, the TCD-based autoregulation index
Mx is the moving-window Pearson correlation between MFV (TCD) and CPP (or MAP, if ICP is unavailable) sampled at slow-wave frequencies (~0.01–0.05 Hz, 5–10 second averages over a 5-minute window).
- Mx ≈ −0.3 to 0.0: intact autoregulation (MFV does not track MAP)
- Mx > +0.3: impaired autoregulation (MFV passively tracks MAP)
- Mx vs CPP curve: U-shape with a minimum at CPPopt
The CPP at which Mx is minimised is the TCD-derived CPPopt: the perfusion pressure at which this patient's autoregulation is most efficient. The Cambridge CPPopt approach formalises this.
Practical CPPopt-by-TCD workflow (when an ICP monitor isn't available or you want a second opinion against PRx):
- Place the TCD probe in a robotic / fixed headframe over the MCA.
- Record continuous MFV synchronously with arterial MAP for ≥ 4 hours.
- Bin MAP / CPP into 5-mmHg windows; compute Mx in each window.
- Fit a parabola to (CPP, Mx); the vertex is CPPopt.
- Re-target MAP so that CPP sits within ±5 mmHg of CPPopt.
Where ICP is available, PRx (ICP–MAP correlation) is preferred because it is closer to the mechanism; Mx is the non-invasive fallback.
9.3 Critical closing pressure (CCP)
CCP is the MAP at which forward CBF ceases. Mathematically, the linear extrapolation of (instantaneous pressure, instantaneous velocity) back to v = 0 returns the closing pressure of the cerebrovascular bed. CCP is composed of ICP plus a wall-tension term reflecting smooth-muscle tone.
- CCP ~ 20–35 mmHg in healthy adults
- CCP rises with raised ICP and with sympathetic activation
- CCP > MAP means no forward flow, i.e., circulatory arrest
CCP from TCD is mostly a research tool, but it is the cleanest way to estimate MAP-opt = CCP + (CPPopt − ICP) when an arterial line and a TCD probe are co-located.
9.4 The bedside synthesis
A pragmatic, PICU-friendly bedside synthesis when ICP is not available:
- Establish the child's baseline MFV in the first 30 minutes after admission, in stable haemodynamics.
- Define a PI ceiling (typically baseline PI + 0.3) above which you will assume ICP has risen.
- If MAP falls and MFV falls proportionally, you are below LLA; give a fluid bolus or vasopressor to lift MAP back into the plateau.
- If MAP rises and MFV rises proportionally, you are above ULA or autoregulation is lost; lower MAP gently (10–15%) and re-measure.
- Document the MFV/MAP couple every nursing shift. A trending impairment (Mx drifting positive) is itself an alert.
Decision support, not a clinical protocol. The TCD-only CPP-titration workflow above is teaching, not measurement. Every threshold is age-, centre-, and patient-dependent. Pair with NIRS, ICP (where available), and clinical exam; defer to your unit's protocols and senior clinical team.
10. Clinical contexts: TCD across acute brain injuries
10.1 Aneurysmal SAH and post-haemorrhagic vasospasm
The historical home of clinical TCD. Vasospasm typically develops between days 3 and 14 post-bleed, peaks around day 7, and resolves over the second-to-third week. TCD is used daily during this window.
- MCA MFV thresholds (adult): < 120 cm/s normal · 120–180 mild · 180–200 moderate · > 200 severe.
- Lindegaard ratio: > 3 confirms vasospasm; > 6 suggests severe.
- Rate of rise > 50 cm/s per 24 h is a stronger predictor of clinical DCI than the absolute number.
- Sensitivity vs DSA is highest for MCA vasospasm (~85%) and lower for ACA and posterior circulation.
- AHA/ASA SAH guidelines include TCD as a recommended monitoring modality.
Pediatric vasospasm is less common (AVM and trauma more frequent than aneurysm) and uses ratios plus within-child trend rather than adult absolute thresholds.
Why care about post-SAH vasospasm at all? Because vasospasm-induced DCI is responsible for roughly 30% of all morbidity after SAH and is, with hydrocephalus, the most reversible cause of secondary injury after the initial bleed. TCD is the only continuous, non-invasive way to track the spasm-to-DCI cascade in real time at the bedside.
10.2 Severe TBI
TCD in TBI is mostly about early ICP triage before an invasive monitor is placed, and about autoregulation monitoring afterwards.
- Pre-hospital and emergency-department TCD identifies abnormal cerebral haemodynamics within minutes of arrival. Tazarourte's pilot and Bouzat's 2016 cohort show that PI > 1.4 or EDV < 25 in the first 8 h predicts poor neurological outcome at 3 months.
- ICP screening: TCD can exclude intracranial hypertension with high negative predictive value when PI is low. Rasulo's 2022 IMPRESSIT-2 multicentre study found the TCD-derived ICP estimate excludes intracranial hypertension with a high NPV, though with poor quantitative concordance (~33%).
- CPPopt by Mx complements PRx and is the standard fallback when ICP is not yet placed.
TCD cannot rule in intracranial hypertension with high specificity. A high PI is suggestive but is also consistent with hypocapnia, sympathetic surge, or sedation. Use it to triage to ICP placement, not to replace it.
10.3 Pediatric arterial ischaemic stroke (AIS)
Continuous TCD in proximal MCA occlusion shows absent flow, low-velocity dampened flow, or post-recanalisation hyperaemia. In children, TCD also helps in:
- Confirming flow re-establishment after thrombolysis or thrombectomy.
- Monitoring for moyamoya progression (rising MFV, ipsilateral hyper-collateralisation).
- Tracking post-recanalisation hyperperfusion that needs BP lowering.
10.4 Hypoxic-ischaemic encephalopathy (HIE): neonatal and post-arrest
In severe HIE, TCD evolves through a sequence:
- Early (hours 0–12): low PSV and low MFV; true low perfusion.
- Reperfusion / luxury phase (12–48 h): high EDV, low PI, high MFV; pathological hyperaemia in a brain whose metabolism has collapsed.
- Recovery or progression: either normalisation, or rising PI signifying oedema and falling CBF.
A persistently low PI (< 0.6) with high diastolic flow at 24–48 h post-arrest is associated with poor neurodevelopmental outcome in pediatric cardiac-arrest survivors.
10.5 Pediatric ECMO
VA-ECMO produces a non-pulsatile circulation; TCD signatures change accordingly. The systolic peak flattens; PI falls toward zero. TCD on ECMO is used to:
- Detect left-ventricular ejection recovery (returning pulsatility).
- Identify emboli (HITS, high-intensity transient signals).
- Monitor flow asymmetry that can predate stroke.
10.6 Meningitis and encephalitis
TCD adds value in two situations: (a) acute intracranial hypertension from cerebral oedema, with high PI and low EDV; (b) vasculitic vasospasm from bacterial or tuberculous meningitis, with high MFV and LR > 3. Both signatures change the threshold for imaging and for ICP placement.
10.7 Brain-death determination
TCD is an ancillary test in the World Brain Death Project framework. The two qualifying patterns are:
- Oscillating / reverberating flow: small forward systolic spikes with reverse end-diastolic flow.
- Systolic spikes only: short forward systolic peaks with no diastolic flow.
A single examination by an experienced operator with confirmation 30 minutes apart, in both anterior and posterior circulations, completes the test. Loss of previously-recorded flow is supportive but not sufficient alone.
10.8 DKA cerebral oedema
A pediatric case where TCD's earliest signs (rising PI before clinical herniation) can change management. Cerebral oedema in DKA classically presents 4–12 h into rehydration. Bedside TCD documenting rising PI prompts mannitol / hypertonic saline before pupillary signs appear.
10.9 Sickle cell disease
The STOP and STOP-2 trials made TCD the standard-of-care screening tool for stroke risk in children with SCD ages 2–16. TAMMV ≥ 200 cm/s triggers chronic transfusion to prevent first stroke; 170–199 is conditional and warrants re-screening.
A pediatric STOP screen requires time-averaged maximum mean velocity (TAMMV), measured with non-imaging blind TCD or with non-angle-corrected TCCD spectral Doppler. Angle-corrected TCCD systematically over-reads TAMMV; do not use angle correction for STOP screens.
11. Multimodal integration: TCD in the MMM/MNM stack
| Pair with… | What you gain | Worked scenario |
|---|---|---|
| ICP | PRx + Mx in parallel; mutual validation of autoregulation; Lindegaard for spasm-vs-hyperaemia | TCD vs ICP vasospasm |
| NIRS / COx | Macrovascular (TCD) + tissue oxygenation (NIRS); discordance signals microvascular shunting | PRx vs COx discordance |
| EEG / qEEG | Vasospasm-induced cortical dysfunction shows up in qEEG before clinical signs | EEG / TCD non-convulsive seizure pair |
| PbtO₂ | Direct microvascular tissue O₂ + macrovascular velocity; gold-standard pair | PbtO₂-CPP titration |
| Clinical exam | Most important pairing; TCD numbers in isolation are dangerous | Always |
12. Setup and technique: a step-by-step
12.1 Equipment
- 2 MHz pulsed-wave probe (blind TCD) or TCCD probe (~ 2–4 MHz with B-mode capability).
- Coupling gel.
- Robotic / fixation headframe (DWL Doppler-Box, Atys Robotic, or Dolphin) for continuous monitoring.
- Synchronised arterial-line pressure and (where present) ICP feeds.
12.2 Transtemporal MCA: the routine view
- Position the patient supine, head neutral, head-of-bed 30°.
- Coupling gel above the zygomatic arch, just anterior to the tragus.
- Probe: 2 MHz pulsed-wave. Initial depth 45 mm (adult) / 30 mm (toddler) / 40 mm (school-age).
- Find the signal: angle anterior and slightly cephalad. Listen for the characteristic systolic "whoosh-thump"; the loudest signal is usually the MCA.
- Confirm with carotid tap: ipsilateral carotid compression in the neck momentarily dampens the MCA envelope and confirms vessel identity.
- Optimise: insonation angle < 30° (cosine error grows fast above 30°). Maximise spectral envelope brightness without overgaining.
- Record PSV, EDV, MFV, PI over ≥ 5 cardiac cycles.
- Repeat contralaterally.
- Lindegaard denominator: switch to submandibular view; ICA at depth ~50–60 mm; compute MFV(MCA) ÷ MFV(ICA).
12.3 Suboccipital basilar
- Head flexed, chin to chest.
- Depth 75–95 mm for the mid-basilar.
- Flow is away from the probe (negative on the envelope); confirm direction.
12.4 Transorbital ophthalmic / ICA siphon
- Use a low mechanical index (< 0.23) to protect the lens.
- Probe directly over the closed eyelid with a generous coupling cushion of gel.
- Depth 40–60 mm for ophthalmic, 60–80 mm for the siphon.
- Note flow direction: ophthalmic toward the probe is normal; reversal suggests proximal ICA stenosis.
12.5 Continuous monitoring
A fixed headframe holds the probe over the MCA for hours. With synchronised arterial pressure recording, you can compute Mx continuously and run a TCD-CPPopt loop without invasive ICP. Pair with NIRS rSO₂ for a "non-invasive autoregulation bundle."
12.6 TCCD vs blind TCD
- TCCD provides B-mode anatomical localisation plus colour Doppler plus angle correction. Preferred in children (thin temporal bone makes B-mode easy) and in adults with poor windows.
- Blind TCD is faster, lower in equipment cost, and the standard tool for STOP screening (which uses non-angle-corrected TAMMV).
13. Pitfalls: operator-dependent, physiology-dependent
- Window quality varies by age, sex, ethnicity. Up to 10% of post-menopausal women have inadequate temporal windows; a contrast agent or a different window can rescue them.
- Hyperaemia mimics vasospasm without the Lindegaard ratio.
- Vessel-diameter change confounds velocity-flow proportionality; this is the entire reason for ratio-based interpretation.
- PI is not ICP. PI rises with anything that increases distal resistance. Use it as a triage, not a measurement.
- Operator dependence: inter-rater reliability is moderate even among trained operators.
- Sedation, anaesthesia, hypothermia lower MFV via CMRO₂ effect (15–25%).
- Hypocapnia raises PI and lowers MFV through hypocapnic vasoconstriction.
- Anaemia raises baseline MFV; every TCD value should be paired with the haemoglobin of the day.
- TCCD angle-correction systematically over-reads TAMMV in SCD; turn it off for STOP screens.
- Probe coupling drift during continuous monitoring shows as gradual envelope dimming; re-aim every 1–2 hours or use a robotic frame.
14. Combine with…
- Lindegaard calculator: distinguishes spasm from hyperaemia.
- Mx, the TCD-based autoregulation index
- Non-invasive ICP: Bellner regression uses PI.
- Integration: TCD vs ICP vasospasm: worked scenario.
- PRx vs COx discordance: non-invasive autoregulation pairings.
- Foundations: autoregulation: Mx, PRx, ORx mechanism.
15. Evidence summary
| Topic | Source | Grade |
|---|---|---|
| Original TCD description | A | |
| Dynamic autoregulation by TCD | B | |
| Lindegaard ratio for vasospasm | A | |
| AAN consensus on TCD applications | expert | |
| Pediatric MCA reference data | B/C | |
| PI for ICP estimation | C | |
| PI is not ICP (pitfall paper) | review | |
| Mx (TCD autoregulation) | B | |
| CPPopt by Mx | B | |
| Critical closing pressure | B | |
| TCD meta-analysis for vasospasm | A | |
| Vasospasm thresholds (re-examined) | B | |
| Pre-hospital TCD in TBI | B | |
| Non-invasive ICP exclusion | B | |
| STOP trial (SCD screening) | A | |
| Pediatric TCD primer | expert | |
| Pediatric ECMO TCD | C | |
| HIE post-arrest TCD prognosis | C | |
| Brain-death determination | expert | |
| TCD waveform analysis (non-invasive ICP) | B/C | |
| Modern TCD review in the ICU | expert | |
| Pediatric MMM consensus | expert |
16. Recent literature (2022–2025)
- Brasil 2022: non-invasive ICP from TCD waveform analysis (Brain4Care-style devices); moving from research into bedside.
- Cardim 2023, Rasulo 2024: multicentre validation of non-invasive ICP estimators against parenchymal probes.
- Figaji 2025 pediatric MMM consensus: formalises TCD as a tier-2 modality in resource-stratified pediatric centres.
- TCCD adoption: colour-coded duplex is replacing blind TCD for routine ICU bedside use, particularly in children.
- Robotic TCD platforms: fixed-frame continuous TCD now standard in many neuro-ICUs; enables Mx, CPPopt-by-TCD, and embolic-signal counting on ECMO.
- Non-invasive ICP exclusion: Rasulo 2022 (IMPRESSIT-2) shows the TCD-derived ICP estimate is a high-NPV rule-out for intracranial hypertension, but with poor quantitative concordance; a low PI is reassuring, while PI > 1.4 alone is not diagnostic.
17. Self-check
References
- Lindegaard KF, Nornes H, Bakke SJ, Sorteberg W, Nakstad P. Cerebral vasospasm diagnosis by means of angiography and blood velocity measurements. Acta Neurochirurgica 1989;100(1-2):12–24. doi:10.1007/BF01405268 link
- Topcuoglu MA, Unal-Cevik I, Arsava EM, Saritas A, Kursun O. Transcranial Doppler in cerebral vasospasm after aneurysmal subarachnoid hemorrhage: thresholds re-examined. Journal of Neuroimaging 2017;27(5):460-467.
- Bellner J, Romner B, Reinstrup P, Kristiansson KA, Ryding E, Brandt L. Transcranial Doppler sonography pulsatility index (PI) reflects intracranial pressure (ICP). Surgical Neurology 2004;62(1):45–51. doi:10.1016/j.surneu.2003.12.007 link
- Rasulo FA, Calza S, Robba C, et al.. Transcranial Doppler as a screening test to exclude intracranial hypertension in brain-injured patients: the IMPRESSIT-2 prospective multicenter international study. Critical Care 2022;26(1):110. doi:10.1186/s13054-022-03978-2 link
- Bouzat P, Almeras L, Manhes P, et al.. Transcranial Doppler to predict neurologic outcome after mild to moderate traumatic brain injury. Anesthesiology 2016;125(2):346-354.
- Kirschen MP, Majmudar T, Beaulieu F, et al.. Transcranial Doppler in pediatric cardiac arrest survivors, association with neurologic outcome. Pediatric Critical Care Medicine 2020;21(5):e221-e229.
- Kontos HA. Validity of cerebral arterial blood flow calculations from velocity measurements. Stroke 1989;20(1):1-3.
- Purkayastha S, Sorond F. Transcranial Doppler ultrasound: technique and application. Seminars in Neurology 2012;32(4):411-420.
- Bathala L, Mehndiratta MM, Sharma VK. Transcranial Doppler: technique and common findings (part 1) and clinical applications (part 2). Annals of Indian Academy of Neurology 2013;16(2-4).
- LaRovere KL, Tasker RC. Transcranial Doppler in critically ill children: a primer. Current Opinion in Pediatrics 2018;30(3):371-377.
- de Riva N, Budohoski KP, Smielewski P, et al.. Transcranial Doppler pulsatility index: what it is and what it is not. Neurocritical Care 2012;17(1):58-66.
- Bode H. Pediatric Applications of Transcranial Doppler Sonography. Springer-Verlag 1988.
- Bode H, Wais U. Age-dependence of flow velocities in basal cerebral arteries. Arch Dis Child 1988;63(6):606–611.
- O'Brien NF. Reference values for cerebral blood flow velocities in critically ill, sedated children. Child's Nervous System 2015;31(12):2269–2276. doi:10.1007/s00381-015-2873-5 link
- LaRovere KL, et al.. Transcranial Doppler in the pediatric intensive care unit. Pediatric Critical Care Medicine 2022.
- Brady KM, Mytar JO, Lee JK, et al.. Monitoring cerebral blood flow pressure autoregulation in pediatric patients during cardiac surgery. Stroke 2010;41(9):1957–1962. doi:10.1161/STROKEAHA.109.575167 link
- Rasulo FA, De Peri E, Lavinio A. Transcranial Doppler ultrasonography in intensive care. European Journal of Anaesthesiology Supplement 2008;25:167–173. doi:10.1017/S0265021507003341 link
- Greer DM, Shemie SD, Lewis A, et al.. Determination of brain death/death by neurologic criteria: the World Brain Death Project. JAMA 2020;324(11):1078-1097.
- Czosnyka M, Smielewski P, Kirkpatrick P, Menon DK, Pickard JD. Monitoring of cerebral autoregulation in head-injured patients. Stroke 1996;27(10):1829–1834.
- Aaslid R, Lindegaard KF, Sorteberg W, Nornes H. Cerebral autoregulation dynamics in humans. Stroke 1989;20(1):45-52.
- Lang EW, Mehdorn HM, Dorsch NW, Czosnyka M. Continuous monitoring of cerebrovascular autoregulation: a validation study. Journal of Neurology, Neurosurgery & Psychiatry 2003;74(8):1053-1059.
- Aries MJH, Czosnyka M, Budohoski KP, et al.. Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury. Critical Care Medicine 2012;40(8):2456–2463. doi:10.1097/CCM.0b013e3182514eb6 link
- Czosnyka M, Smielewski P, Kirkpatrick P, Laing RJ, Menon D, Pickard JD. Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery 1997;41(1):11–17.
- Donnelly J, Czosnyka M, Adams H, et al.. Individualizing thresholds of cerebral perfusion pressure using estimated limits of autoregulation. Critical Care Medicine 2017;45(9):1464-1471.
- Varsos GV, Richards H, Kasprowicz M, Schmidt EA, Brady KM, Czosnyka M. Critical closing pressure determined with a model of cerebrovascular impedance. Journal of Cerebral Blood Flow & Metabolism 2013;33(2):235-243.
- Mastantuono JM, Combescure C, Elia N, Tramer MR, Lysakowski C. Transcranial Doppler in the diagnosis of cerebral vasospasm: an updated meta-analysis. Critical Care Medicine 2018;46(10):1665-1672.
- Connolly ES, Rabinstein AA, Carhuapoma JR, et al.. Guidelines for the management of aneurysmal subarachnoid hemorrhage, AHA/ASA. Stroke 2012;43(6):1711-1737.
- Tazarourte K, Atchabahian A, Tourtier JP, et al.. Pre-hospital transcranial Doppler in severe traumatic brain injury: a pilot study. Acta Anaesthesiologica Scandinavica 2011;55(4):422-428.
- LaRovere KL, Vonberg FW, Prabhu SP, et al.. Patterns of head computed tomography abnormalities during pediatric ECMO and association with outcomes. Pediatric Neurology 2017;73:64-70.
- Tunkel AR, Hartman BJ, Kaplan SL, et al.. Practice guidelines for the management of bacterial meningitis (IDSA). Clinical Infectious Diseases 2004;39(9):1267–1284.
- Glaser N, Barnett P, McCaslin I, et al.. Risk factors for cerebral edema in children with diabetic ketoacidosis. NEJM 2001;344(4):264–269.
- Muir AB, Quisling RG, Yang MCK, Rosenbloom AL. Cerebral edema in childhood diabetic ketoacidosis: natural history, radiographic findings, and early identification. Diabetes Care 2004;27(7):1541–1546.
- Adams RJ, McKie VC, Hsu L, et al.. Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. NEJM 1998;339(1):5–11.
- Adams RJ, Brambilla D, STOP-2 Investigators. Discontinuing prophylactic transfusions used to prevent stroke in sickle cell disease. NEJM 2005;353(26):2769–2778.
- Figaji AA, Tasker RC, Bell MJ, Kochanek PM. Pediatric multimodal monitoring consensus update, practical algorithms for resource-stratified centers. Intensive Care Medicine, Paediatric and Neonatal 2025.
- Helbok R, Tasker RC, Kochanek PM, Bell MJ. Pediatric multimodal monitoring: where are we and where do we go?. Pediatric Critical Care Medicine 2024.
- Tasker RC, LaRovere KL, Riviello JJ, et al.. Pediatric multimodal neuromonitoring: international Delphi consensus. Pediatric Critical Care Medicine 2023.
- Vinciguerra L, Bosel J. Noninvasive neuromonitoring: current utility in subarachnoid hemorrhage, traumatic brain injury, and stroke. Neurocritical Care 2017;27(1):122-140.
- Aaslid R, Markwalder TM, Nornes H. Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries. Journal of Neurosurgery 1982;57(6):769–774. doi:10.3171/jns.1982.57.6.0769 link
- Sloan MA, Alexandrov AV, Tegeler CH, et al.. Assessment: transcranial Doppler ultrasonography: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2004;62(9):1468–1481. doi:10.1212/wnl.62.9.1468 link
- Brasil S, Solla DJF, Nogueira RC, Teixeira MJ, Malbouisson LMS, Paiva WS. Intracranial compliance and cerebral perfusion: novel non-invasive assessment using waveform analysis. Brain Sciences 2022;12(11):1559.
- Cardim D, Robba C, Czosnyka M, et al.. Non-invasive ICP estimation: an updated review. J Clin Monit Comput 2023.
- Rasulo FA, Brasil S, Andrade R, Robba C. Non-invasive ICP estimation by Brain4Care: prospective validation across centers. Neurocritical Care 2024.