The Monro-Kellie doctrine
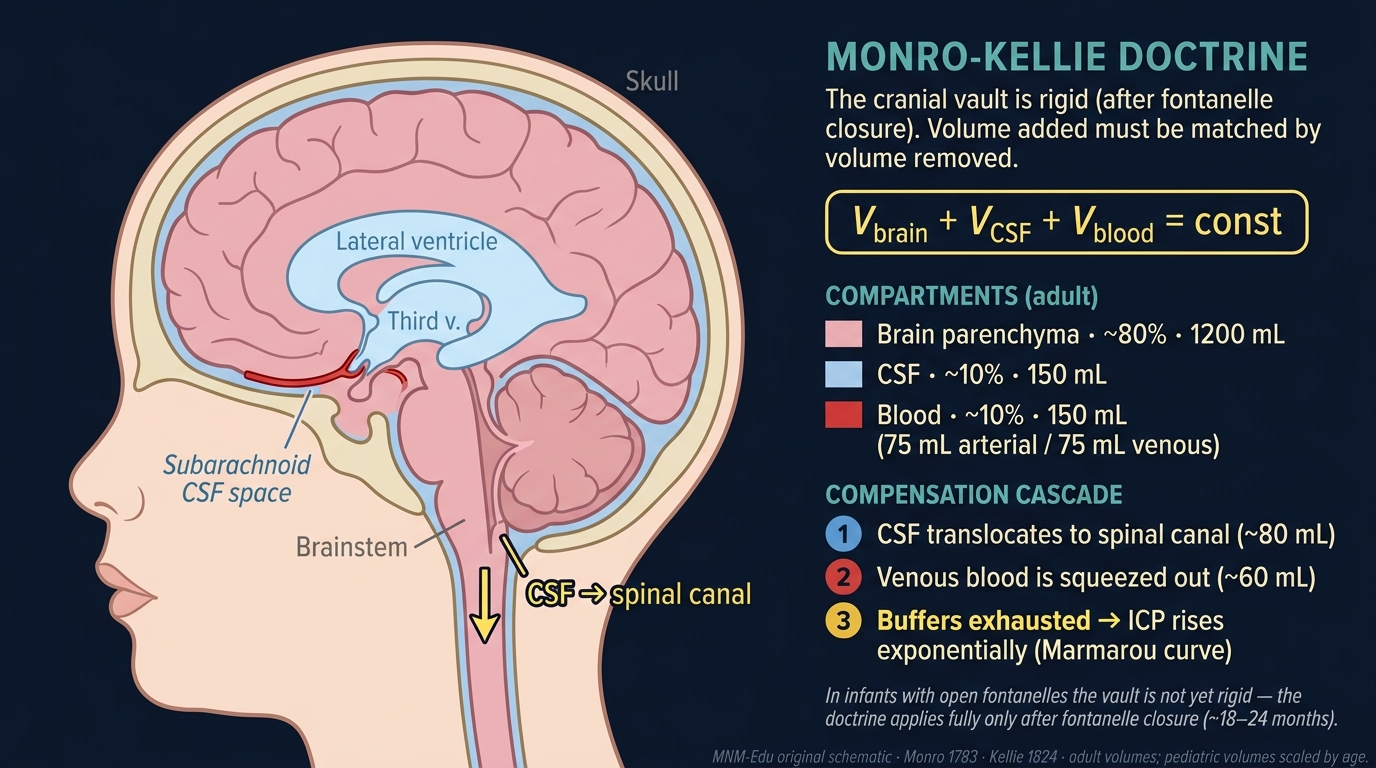
The cranial vault is rigid. Anything that adds volume must be paid for somewhere, first by CSF, then by blood, then by ICP.
1. Bedside vignette: small volume, big spike
A 6-year-old with medulloblastoma develops increasing morning headaches and vomiting. The baseline ICP from the ventricular reservoir at clinic last week was 12 mmHg with RAP 0.4, no waveform abnormalities. On admission she undergoes a stable anaesthetic. Halfway through scan transfer her ICP suddenly spikes from 14 to 32 mmHg during a routine 5 mL CSF aspiration delay; pupils stay equal; ICP recovers over 4 minutes to 22.
What happened? The slow tumour growth over the past week has moved the operating point up the Marmarou exponential. A volume change that was unimportant last month is now happening near the knee of the curve. The CSF buffer is nearly exhausted; the venous reserve is partly used; the next mL costs many mmHg. RAP redrawn the next morning is 0.8, the patient is on the steep segment. The case for urgent CSF diversion is now numerical, not just clinical.
This is what the Monro-Kellie doctrine looks like at the bedside: not in static numbers, but in how much one more mL costs.
2. The three compartments
A child's skull begins as flexible plates joined by sutures and fontanelles, then ossifies through childhood. By school age, the cranial vault is a rigid box. Volume in must equal volume out, or pressure rises.
The cranial vault, about 1500 mL in an adult, holds three things in fixed total:
- Brain parenchyma, ~80% (~1200 mL): cells + interstitial fluid + myelin.
- Blood (mostly venous), ~10% (~150 mL): the arterial side is small; most blood at any moment sits in the veins and venous sinuses.
- CSF, ~10% (~150 mL): made by the choroid plexus at ~500 mL/day; whole CSF volume turns over 3–4 times a day.
Add to one and the body must subtract from another, or pressure rises.
3. Compensatory sequence: CSF, venous, then crisis
When something starts to grow (tumour, haematoma, contusion oedema, abscess, hydrocephalus):
- CSF first. The cheapest buffer. CSF translocates from the cranial subarachnoid space into the spinal canal via the foramen magnum. Up to ~80 mL of pathological volume is absorbed this way without ICP rising at all.
- Venous blood second. Once CSF capacity is exhausted, the dural venous sinuses and cerebral veins compress. Cerebral venous outflow speeds up. Another ~60 mL absorbed.
- No more buffer. Now ICP climbs steeply along the Marmarou exponential: every additional mL produces a much larger pressure jump than the last one.
Why the first 5 mL is free and the last 5 mL is fatal. Compliance falls exponentially. The Marmarou pressure-volume index (PVI), the volume change required to raise ICP by a factor of 10, is ~20 mL in adults. Below the knee of the curve, +1 mL is harmless; near the top, +1 mL doubles ICP.
4. Why the curve goes vertical: Marmarou exponential and compliance exhaustion
The pressure-volume relationship in the cranium is approximately:
with local elastance (dP/dV) climbing as you move up the curve. At ICP 10, +1 mL barely moves the needle. At ICP 30, the same +1 mL adds several mmHg. The Marmarou exponential is the mathematical statement of the Monro-Kellie doctrine; the foundation page on the pressure-volume curve covers the math in detail.
RAP operationalises compliance at the bedside: it is the moving Pearson correlation between ICP pulse amplitude (AMP) and mean ICP, computed over a 4-minute window.
- RAP < 0.3: flat segment of the PV curve; reserve intact.
- 0.3–0.6: borderline.
- 0.6–0.9: steep segment; low compensatory reserve.
- Paradoxical fall toward 0 at high ICP: the brain can no longer transmit the pulse; terminal decompensation.
5. Why it matters at the bedside
The Monro-Kellie doctrine has direct management consequences:
- Head-up 30° improves jugular outflow; reduces venous compartment volume.
- Avoiding tight cervical collars preserves outflow.
- Sedation and analgesia lower CMRO₂ and indirectly trim cerebral blood volume.
- Brief hypocapnia is a vasoconstrictive lever (acute use only; see CO₂ reactivity page).
- Osmotherapy (HTS or mannitol) draws water out of the brain compartment.
- CSF drainage via EVD is the fastest tool when the CSF compartment can be tapped.
- Decompressive craniectomy removes the rigid-box constraint: the new compliant compartment buys the brain time, though outcome data are mixed in pediatric severe TBI.
Open fontanelles compensate, but only slowly. A neonate with a slowly growing tumour or chronic hydrocephalus may compensate by skull expansion (head circumference rising) for weeks. An acute insult, haematoma, severe oedema, status epilepticus, overwhelms even an open fontanelle in hours because the elastic limit of skin and dura is far less than that of the volume buffer the suture lines provide. Do not be reassured by a soft fontanelle in an acutely ill child. Anterior fontanelle closes ~12–18 months; posterior ~2–3 months. Sutures fuse by ~5 years.
6. Pattern library
- RAP rising as ICP rises: classic decompensation; compliance falling, operating point moving up the curve.
- RAP high but ICP stable: stable compensation at a low-reserve point; small additional insult will cost more.
- RAP collapsing at very high ICP: AMP can no longer follow mean ICP; pulse transmission is failing. Bad sign.
- Plateau waves (Lundberg A): trapezoidal envelope, 60-second rise, 5–20-minute plateau at very high ICP, 60-second fall. Appear when low compliance plus marginal CPP plus active vasomotor align.
- B-waves: rhythmic 0.5–2/min, 5–20 mmHg amplitude; associated with low compliance and sleep cycles.
7. Pitfalls
- Reading ICP without context: ICP 18 with RAP 0.2 is different from ICP 18 with RAP 0.85.
- Forgetting venous outflow: tight neck lines, cervical collar misuse, prone positioning all raise CVP and therefore ICP.
- Reassurance from open fontanelle: chronic compensation, not acute buffer.
- Treating absolute number without trend: ICP creeping from 12 to 18 over 6 hours matters even if both are "normal".
- Mannitol after BBB failure: in late TBI or stroke, mannitol can redistribute and worsen oedema.
8. Combine with…
- Modality: ICP: the bedside readout that the doctrine predicts.
- Modality: RAP: the operational compliance index.
- Modality: CPP: MAP − ICP, the perfusion correlate.
- Foundation: pressure-volume curve: the maths behind compliance exhaustion.
- Foundation: pediatric physiology: fontanelle and skull development.
- Integration: osmotherapy ICP NIRS: a worked scenario.
9. Why rigidity matters
The skull's mechanical stiffness is what makes pressure-volume relationships in the cranium so steep compared to other compartments. The rigid box also means that venous pressure matters: anything that raises CVP (PEEP, head-down positioning, jugular obstruction) raises ICP through impeded outflow.
10. Compartments and pathology
- Brain oedema (vasogenic, cytotoxic, osmotic) raises parenchymal volume.
- Haematoma (intracerebral, subdural, epidural) raises blood compartment.
- Hydrocephalus raises CSF compartment.
- Mass lesion (tumour, abscess) follows the same logic.
In each case the compensatory window is the same: first CSF, then venous, then crisis.
11. The hidden compartment
In open systems (decompressive craniectomy, large skull fractures), the rigid-box assumption breaks down. ICP becomes a function of external atmospheric pressure plus tissue pressure across the bone defect. This is part of the rationale for craniectomy in refractory hypertension.
12. Mokri 2001, the contemporary statement
Mokri reformulates Monro-Kellie for the era of CSF leaks: when CSF volume falls (e.g., spontaneous intracranial hypotension), the body compensates by expanding venous volume, producing the venous engorgement and pachymeningeal enhancement seen on MRI. The doctrine works in both directions.
13. Practical bedside application
The doctrine is why:
- Head-up 30° matters (improves jugular outflow).
- Avoiding tight cervical collars matters (preserves outflow).
- PEEP matters less in stiff lungs (low transmission).
- EVD drainage is fast and effective when CSF compartment is accessible.
- Decompressive craniectomy removes the rigid-box constraint.
14. Evidence summary
| Topic | Source | Grade |
|---|---|---|
| Original doctrine | foundational | |
| Marmarou exponential | A | |
| Avezaat pulsatility-pressure | B | |
| RAP introduction | B | |
| RAP modern use | B | |
| RAP at very high ICP | C | |
| Mokri reformulation | review | |
| Decompressive craniectomy (adult) | A | |
| Venous outflow / CVP effects | C | |
| Pediatric TBI guideline | expert |
15. Self-check
References
- Monro A. Observations on the structure and functions of the nervous system. Edinburgh: Creech & Johnson 1783.
- Kellie G. An account of the appearances observed in the dissection of two of the three individuals presumed to have perished in the storm of the 3rd, and whose bodies were discovered in the vicinity of Leith on the morning of the 4th of November 1821. Transactions of the Medico-Chirurgical Society of Edinburgh 1824;1:84–169.
- Marmarou A, Shulman K, Rosende RM. A nonlinear analysis of the cerebrospinal fluid system and intracranial pressure dynamics. Journal of Neurosurgery 1978;48(3):332–344. doi:10.3171/jns.1978.48.3.0332 link
- Kim DJ, Carrera E, Czosnyka M, Keong N, Smielewski P, Pickard JD. Index of cerebrospinal compensatory reserve in hydrocephalus. Neurosurgery 2009;64(3):494–501.
- Avezaat CJJ, van Eijndhoven JHM, Wyper DJ. Cerebrospinal fluid pulse pressure and intracranial volume-pressure relationships. Journal of Neurology, Neurosurgery, and Psychiatry 1979;42(8):687–700. doi:10.1136/jnnp.42.8.687 link
- Czosnyka M, Guazzo E, Whitehouse M, et al.. Significance of intracranial pressure waveform analysis after head injury. Acta Neurochirurgica 1996;138(5):531–541. doi:10.1007/BF01411173 link
- Howells T, Johnson U, McKelvey T, Enblad P. An optimal frequency range for the analysis of pressure reactivity. Journal of Clinical Monitoring and Computing 2017;31(1):85–93.
- Kazimierska A, Kasprowicz M, Czosnyka M, et al.. Compliance of the cerebrospinal space: comparison of three methods. Acta Neurochirurgica 2021;163(7):1979–1989. doi:10.1007/s00701-021-04834-y link
- Hutchinson PJ, Kolias AG, Timofeev IS, et al.. Trial of decompressive craniectomy for traumatic intracranial hypertension. New England Journal of Medicine 2016;375(12):1119–1130. doi:10.1056/NEJMoa1605215 link
- Cooper DJ, Rosenfeld JV, Murray L, et al.. Decompressive craniectomy in diffuse traumatic brain injury. New England Journal of Medicine 2011;364(16):1493–1502. doi:10.1056/NEJMoa1102077 link
- Kochanek PM, Tasker RC, Carney N, et al.. Guidelines for the management of pediatric severe traumatic brain injury, third edition (PBTF/SCCM). Pediatric Critical Care Medicine 2019;20(3S):S1-S82.
- Lundberg N. Continuous recording and control of ventricular fluid pressure in neurosurgical practice. Acta Psychiatrica et Neurologica Scandinavica 1960;36(Suppl 149):1–193.
- Czosnyka M, Smielewski P, Piechnik S, et al.. Hemodynamic characterization of intracranial pressure plateau waves in head-injury patients. Journal of Neurosurgery 1999;91(1):11–19. doi:10.3171/jns.1999.91.1.0011 link
- Caricato A, Conti G, Della Corte F, et al.. Effects of PEEP on the intracranial system of patients with head injury and subarachnoid hemorrhage: the role of respiratory system compliance. Journal of Trauma 2005;58(3):571–576. doi:10.1097/01.ta.0000152806.19198.db link
- Mokri B. The Monro-Kellie hypothesis: applications in CSF volume depletion. Neurology 2001;56(12):1746–1748. doi:10.1212/wnl.56.12.1746 link