Quantitative pupillometry and the Neurological Pupil index
A handheld infrared camera that turns the pupillary light reflex into a numerical index (NPi 0 to 5) plus constriction velocity and latency. Pediatric-first, with the ORANGE multicentre data context.
1. Bedside vignettes: why this matters in the PICU
Vignette A. The 9-year-old TBI on Q1 hour pupil checks
A 9-year-old is admitted with severe TBI after a fall, ICP monitor in place, GCS 6T. The bedside flow sheet shows hourly pen-torch pupillary exams (4 mm bilateral, brisk) for 8 hours. The pupillometer is added to the routine at hour 9. The first NPi readings are 4.2 on the right, 4.1 on the left, normal. Six hours later: right NPi 3.1, left NPi 4.0 (asymmetry > 0.7 is abnormal even when both are above 3). The clinical pen-torch exam still reads "4 mm bilateral, brisk." An urgent CT shows new right uncal swelling and early midline shift. The team hyperosmolises and accelerates the decompressive craniectomy decision. The pupillometer caught it before the eye did.
Vignette B. The 5-year-old after cardiac arrest, day 3
A 5-year-old is on day 3 after an out-of-hospital arrest, normothermic, sedation off. Bilateral NPi = 0 with absent constriction velocity, latency unrecordable. Bedside FOUR score = 1 (motor only, extensor). SSEP shows bilateral absent N20. MRI shows diffuse cortical and basal ganglia injury. The multimodal prognostication framework (NPi + FOUR + SSEP + MRI + 72 h post-arrest timing) supports the conversation with the family about prognosis. No single number, including NPi 0, is enough by itself; the value of the pupillometer here is one quantitatively reliable leg of the multimodal prognostication stool.
Vignette C. The 2-month-old with normal NPi and dilated pupils on hyoscine
A 2-month-old with bronchiolitis is on a high-dose hyoscine patch for secretions and on a one-time dose of glycopyrrolate before fundoscopy. Hours later her pupils measure 6 mm bilateral and "non-reactive" on pen-torch. The team panics, calling neurology. The pupillometer reads: max pupil 6.2 mm, min 6.0 mm, CV 0.0 mm/s, NPi 0. But the brainstem reflexes (corneals, cough, gag) are intact, the GCS is at her pre-illness baseline, and there is no other concerning sign. NPi 0 from pharmacological mydriasis looks identical to NPi 0 from CN III failure. Always interrogate the drug list before interpreting a flat pupillometer trace.
2. What pupillometry is, and what it is not
The pupillometer is a handheld infrared video camera that delivers a calibrated light pulse (typically 1000 lux, 0.8 s) to the pupil and records the diameter at high frame rate (30 to 60 fps) for the constriction and dilation phases. The device extracts:
- Maximum pupil diameter (MAX): pre-stimulus baseline, in mm.
- Minimum pupil diameter (MIN): peak constriction, in mm.
- Percent change (% CH): (MAX − MIN) / MAX × 100.
- Constriction velocity (CV): average rate of constriction in mm/s.
- Latency (LAT): time from stimulus onset to start of constriction, in ms.
- Dilation velocity (DV): average rate of return to baseline, in mm/s.
- Neurological Pupil index (NPi): a proprietary algorithm that combines the above into a single 0 to 5 score with reference to a healthy-population model.
The NPi is not the same as constriction velocity, and the two move independently. A blown CN III pupil shows NPi 0 with CV 0; a healthy pupil shows NPi 4 to 5 with CV ~1 to 2 mm/s; an early-warning pupil with subtle CN III compromise may show NPi 2.5 to 3.0 with CV slightly reduced and LAT slightly prolonged before the pen-torch exam picks up anything. The 0.7 unit asymmetry threshold is the most sensitive single signal of unilateral early uncal herniation.
Two things follow.
Pupillometry quantifies what your pen-torch already does. The pen-torch returns "brisk / sluggish / fixed" with moderate inter-rater agreement (kappa ~0.4 to 0.6). The pupillometer returns continuous numbers with near-zero inter-rater variability (kappa > 0.9). The qualitative-to-quantitative move is the single biggest reason to add a pupillometer to your unit.
The NPi is calibrated against an adult healthy population. Pediatric reference data (Freeman 2020, Kerscher 2023, Jiang 2023, Kirschen 2025) suggest the adult thresholds (NPi < 3 abnormal) hold reasonably in children > 1 month, but normative ranges in neonates and preterm infants are different and a "low" NPi in the first weeks of life may not have the same prognostic weight.
Trend over absolute. A single NPi of 3.2 in a stable post-op patient is reassurance. A series of NPi values trending 4.1 → 3.8 → 3.5 → 3.2 over 4 hours in a TBI patient on the same observer's measurements is a deteriorating exam, even though all four numbers are technically "normal" by some thresholds. The pupillometer is at its best when it is used routinely (Q1 to Q4 hour), not as a one-off curiosity.
Pediatric normative data are still maturing. Freeman 2020 reported pediatric NPi 95% reference range 3.2 to 4.7 in healthy children, similar to adult ranges. Kerscher 2023 confirmed the abnormal threshold (NPi < 3) in pediatric TBI. Neonatal pupillometry is investigational (small pupils, immature parasympathetic, technical challenges); use only in centres with research protocols.
3. Anatomy and pathway: from light to pupil
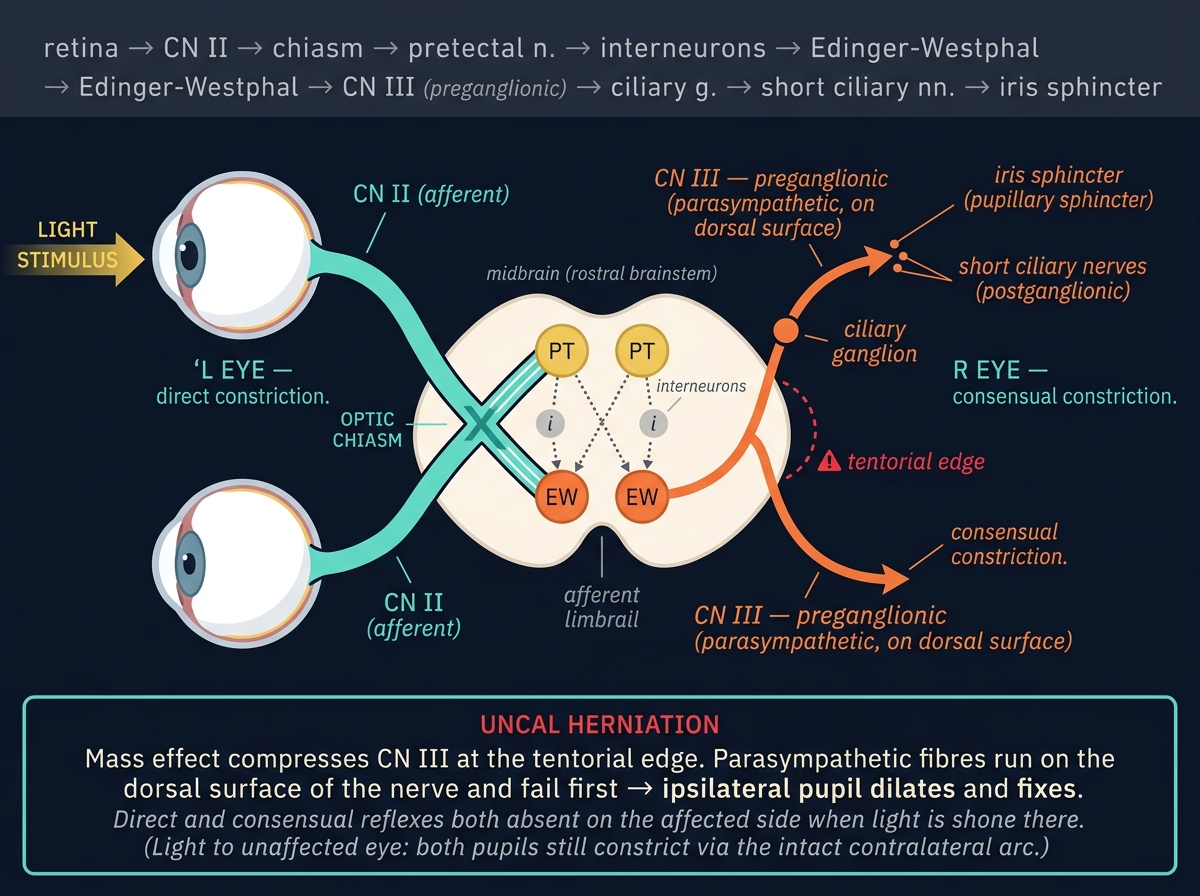
The pupillary light reflex traverses a four-neuron arc.
- Afferent (CN II): retinal ganglion cells → optic nerve → optic chiasm → optic tract → pretectal nuclei of the midbrain.
- Inter-neuron: pretectal nucleus → bilateral Edinger-Westphal nuclei (which is why the consensual response exists).
- Efferent parasympathetic (CN III): Edinger-Westphal nucleus → CN III preganglionic fibres → ciliary ganglion → short ciliary nerves → iris sphincter (constriction).
- Efferent sympathetic: descending hypothalamic → ciliospinal centre (C8 to T2) → superior cervical ganglion → long ciliary nerves → iris dilator (dilation, also opposed when constriction is forced by light).
Where the lesion sits determines the pupillometer pattern.
| Lesion site | NPi | CV | LAT | Asymmetry |
|---|---|---|---|---|
| Optic nerve (CN II) | Slightly low | Reduced afferent gain | Normal | Direct affected only, consensual preserved (Marcus Gunn) |
| Midbrain pretectum | Variable | Reduced | Normal | Bilateral |
| Edinger-Westphal / CN III nucleus | Low to 0 | Low to 0 | Prolonged | Often bilateral with progression |
| CN III axonal compression (uncal herniation) | Falls before pen-torch picks up | Falls early | Lengthens | Unilateral, then bilateral as herniation worsens |
| Ciliary ganglion / parasympathetic axons | Low | Low | Prolonged | Often unilateral (Adie's, surgical) |
| Pharmacological mydriasis | 0 if anticholinergic | 0 | unrecordable | Bilateral if systemic; unilateral if topical |
This anatomy is why a unilateral falling NPi in a TBI patient is the bedside signature of evolving uncal herniation hours before the pen-torch sees it. The pupillometer detects subtle CV reduction and LAT prolongation while the visual estimate of "pupil size and reactivity" still reads normal.
4. The signal: what a typical NPi waveform looks like
A normal trace has six readable features.
- A stable MAX pre-stimulus baseline, recorded over ~1 s before the light pulse.
- A short latency (200 to 300 ms) between stimulus onset and the start of constriction. LAT > 350 ms is abnormal.
- A brisk constriction phase at CV ~1 to 2 mm/s. CV < 0.6 mm/s is abnormal.
- A deep nadir (MIN) giving > 10% change from MAX in healthy adults, > 13% in healthy children.
- A smooth re-dilation phase at DV ~0.5 to 1.0 mm/s. Abnormally fast dilation can suggest sympathetic overactivity (sepsis, pain).
- A return to baseline within 3 to 5 s.
In a patient with early uncal herniation, the latency and CV are usually the first to drift before the MAX, MIN, or % CH show change. This is the basis of the NPi's early-warning utility: it composites these subtle changes into a single trending number.
Latency is the most sensitive single number on the trace for evolving CN III dysfunction. A LAT > 350 ms with otherwise normal MAX, MIN, and CV is the earliest pupillometer marker of CN III compromise in some series.
5. The numbers to record
| Variable | Symbol | What it tells you |
|---|---|---|
| Neurological Pupil index | NPi (0 to 5) | The headline summary score; trend matters more than absolute |
| Constriction velocity | CV (mm/s) | The most physically interpretable number; falls with CN III compromise |
| Latency | LAT (ms) | Often the earliest sign of subtle compromise |
| Maximum diameter | MAX (mm) | Pre-stimulus baseline; rises with sympathetic activation or anticholinergics |
| Minimum diameter | MIN (mm) | Depth of constriction; reflects functional sphincter mass |
| Percent change | % CH | (MAX − MIN) / MAX × 100; alternative summary measure |
| Dilation velocity | DV (mm/s) | Re-dilation kinetics; fast DV suggests sympathetic overactivity |
| Asymmetry | Δ NPi, Δ CV between sides | Asymmetry > 0.7 in NPi is abnormal even if both sides are individually within range |
Record both sides, every time, in the same order. Most units document the trend graphically on the bedside chart alongside ICP, CPP, and GCS.
6. What is normal? Age-banded reference values
| Age | NPi (mean, 95% CI) | CV (mean, mm/s) | LAT (ms) | MAX (mm, ambient) |
|---|---|---|---|---|
| Preterm (< 37 wk) | research only; not validated | n/a | n/a | n/a |
| Term newborn | research only; small numbers | n/a | n/a | 2.0 to 3.5 |
| 1 to 6 months | 3.0 to 4.5 (very limited data) | ~1.0 | 250 to 350 | 2.5 to 4.0 |
| 6 months to 2 years | 3.5 to 4.7 | 1.0 to 1.5 | 220 to 320 | 3.0 to 4.5 |
| 2 to 12 years | 3.5 to 4.8 | 1.2 to 1.8 | 200 to 300 | 3.5 to 5.5 |
| Adolescents and adults | 3.5 to 4.7 | 1.0 to 2.0 | 200 to 300 | 3.0 to 6.0 |
Sources: . Pediatric data are still emerging; the adult thresholds (NPi < 3 abnormal, < 2 strongly abnormal) appear to hold for children > 6 months.
Three child-specific calibrations.
- Sleeping infants have small, slowly-reactive pupils that may read "abnormal" by adult criteria. Always document state (awake / asleep / sedated) at the time of measurement.
- Eye colour and iris pigmentation affect both visual estimate and infrared video; the pupillometer is more robust to pigmentation than the pen-torch but is not immune.
- A toddler will fight you. Brief, single-pass measurements with the eyecup held gently are better than prolonged attempts; let the parent be present.
7. What is abnormal? Pattern library
| Pattern | Bedside meaning | What to do |
|---|---|---|
| NPi 3.5 to 5, symmetric | Normal | Continue routine |
| NPi 2 to 3, symmetric | Sluggish; subtle compromise OR sedation effect | Recheck in 1 h; verify sedation contribution |
| NPi < 2 either side | Strongly abnormal | Imaging; consider escalation |
| NPi 0 with absent CV | Functional CN III absent (structural or pharmacological) | Interrogate drug list; structural workup if unexplained |
| Asymmetry Δ NPi > 0.7 | Unilateral pathology evolving | Recheck CT; consider lateralising lesion |
| Falling NPi trend (Δ > 0.5 over 4 h) | Subacute deterioration | Recheck imaging and labs; escalate |
| NPi normal but CV very low | Subtle parasympathetic compromise | Trend; pair with exam |
| MAX large, CV low, LAT prolonged | Anticholinergic effect (atropine, scopolamine, ipratropium) | Drug review; expect recovery |
| MAX small, CV normal, NPi normal | Opioid or pontine lesion | Clinical correlation |
Decision tree: "what is the NPi telling me?"
flowchart TD
Reading[Pupillometer reading] --> Abn{NPi < 3 or asymmetry > 0.7?}
Abn -->|No| Normal[Continue routine]
Abn -->|Yes| Drug{New anticholinergic or opioid?}
Drug -->|Yes| Pharm[Pharmacological; reassess]
Drug -->|No| Trend{Trend over last 4 h?}
Trend -->|Stable abnormal| Care[Document, increase frequency]
Trend -->|Falling| Esc[Escalate: imaging, ICP, NSG]
Esc --> Action[CT, hypertonic, head up, NSG]
8. Try it: interactive widgets
9. Pupillometry-driven management
The pupillometer does not titrate a single drug or pressure on its own. It triggers decisions.
9.1 ICP and CPP
A falling NPi in a TBI patient with an ICP monitor in place forces a recheck of ICP, CPP, sedation, head position, PaCO2, temperature, and serum sodium. A falling NPi in a patient without a monitor strongly justifies placing one (or, at minimum, urgent imaging).
9.2 Hyperosmolar therapy
A falling NPi with an ICP > 20 mmHg (all pediatric ages, Kochanek 2019) supports an immediate hypertonic saline or mannitol bolus. The NPi response after osmotherapy can be re-checked at 30 to 60 min: a recovering NPi is reassurance; a continuing fall mandates escalation.
9.3 Sedation titration
A patient on opioid infusions may have small pupils with preserved NPi; a patient on benzodiazepines may show slightly low NPi (2.5 to 3) without structural cause. Sedation-induced low NPi tends to recover with a daily sedation hold; structural low NPi does not. The daily sedation hold has dual purpose: it lets the clinical exam and the pupillometer both report on the brain rather than the drug.
9.4 Prognostication after cardiac arrest
In the multimodal prognostication framework, persistent NPi 0 bilaterally at 72 h post-arrest, combined with bilateral absent SSEP N20, a markedly suppressed EEG, and diffuse cortical injury on MRI, is strongly associated with poor neurological outcome. No single modality, including NPi, is sufficient for prognostication; the framework requires concordance across at least 3 modalities.
Teaching, not protocol. The decision pathways on this page are teaching algorithms. Every threshold (NPi 3, asymmetry 0.7, Δ over 4 h) is centre-, age-, and patient-specific. Pair the pupillometer with clinical exam, ICP, NIRS, EEG, and imaging; defer to your unit's protocols and senior clinical team.
10. Clinical contexts: NPi across acute brain injuries
10.1 Severe TBI
The primary published indication for pupillometry. Two registry datasets:
- ORANGE adult multicentre cohort (Oddo 2023): NPi < 3 sustained > 1 h was associated with poor outcome (mRS 4 to 6) independently of GCS and CT findings.
- Petrosino 2025 ORANGE pediatric pilot: smaller cohort but consistent direction; falling NPi over 6 to 12 h preceded clinical herniation by a median 9 h.
In pediatric severe TBI, the pupillometer adds quantitative early warning to the BTF / pBTF management bundle. It does not replace ICP monitoring but it is a useful adjunct for the patient whose ICP monitor is delayed.
10.2 Aneurysmal SAH
NPi is added value in SAH for two reasons. First, early signs of evolving hydrocephalus or rebleed are caught earlier than by pen-torch. Second, in the DCI window (days 3 to 14), a unilateral fall in NPi often precedes the focal neurological deficit that classically defines clinical DCI. Pair with daily TCD and qEEG.
10.3 Pediatric AIS
In a child receiving thrombectomy or thrombolysis for arterial ischaemic stroke, the pupillometer monitors for post-recanalisation oedema and the rare but devastating hyperperfusion haemorrhage. A new asymmetry > 0.7 or a falling NPi within 24 h of recanalisation triggers BP review and urgent imaging.
10.4 HIE and post-cardiac arrest
The pupillometer's role here is prognostic, not real-time titration. Bilateral NPi 0 at 72 h post-arrest in a normothermic, sedation-free patient is one leg of the multimodal prognostication framework. Do not prognosticate during hypothermia or in the first 72 hours; sedation, hypothermia, and metabolic confounders depress NPi reversibly.
10.5 Pediatric ECMO
VA-ECMO carries 5 to 15% risk of acute neurological injury (stroke, ICH, anoxic brain injury). Daily pupillometry is part of the ELSO neurological surveillance bundle. A new asymmetry > 0.7 or a falling NPi triggers head CT, fontanelle ultrasound, or MRI. The technical challenge: the constant ECMO circuit traffic around the bed and frequent transfers make routine pupillometry harder than in a stable ICU patient.
10.6 Meningitis and encephalitis
In bacterial meningitis with evolving cerebral oedema or vasculitic vasospasm, the pupillometer can catch early herniation signs in a patient where the clinical exam is depressed by the underlying illness. A falling NPi in this context warrants repeat imaging and consideration of EVD or ICP monitoring.
10.7 Brain-death determination
Pupillometry is not a brain-death determination tool by itself. It is, however, a useful adjunct that documents the absence of any constriction response with a number rather than a qualitative descriptor. NPi 0 with CV 0 bilaterally adds quantitative weight to the clinical brain-death exam. Pediatric brain-death criteria still require the standard clinical exam + apnoea test repeated at the age-appropriate interval.
10.8 DKA cerebral oedema
A child being rehydrated for DKA whose NPi drops 0.7 or more units between hours 4 and 24 of treatment should prompt cerebral oedema treatment (mannitol or hypertonic saline) regardless of the absolute value. The pupillometer here gives a quantitative early-warning signal that supplements clinical vigilance for headache, vomiting, bradycardia, and hypertension.
10.9 Refractory status epilepticus
In a child on continuous infusion (midazolam, pentobarbital, ketamine) for refractory status, pupillometry can detect oversedation (very low NPi, very low CV, slow DV) and titrate downward, especially when EEG burst suppression is the chosen target and the bedside exam is unreliable.
11. Multimodal integration: pupillometry in the MMM/MNM stack
| Pair with… | What you gain | Worked scenario |
|---|---|---|
| Clinical exam | Quantitative complement to GCS / FOUR | Pen-torch reads "brisk"; pupillometer catches subtle CV decline |
| ICP / CPP | Pupillometer change with stable ICP suggests CN III lesion separate from raised pressure | TBI with stable ICP and new NPi asymmetry: structural workup |
| CT / MRI | Pupillometer triggers imaging; imaging refines | New asymmetry > 0.7 → CT shows uncal swelling |
| TCD | Two early-warning indices: NPi and PI both rise before clinical herniation | TBI: NPi falling and TCD PI rising signal shared underlying ICP rise |
| SSEP / EP | Multimodal prognostication after cardiac arrest | NPi 0 + bilateral absent N20 + suppressed EEG: poor prognosis |
| EEG / qEEG | NPi catches structural; EEG catches electrical | SE refractory to first-line: pair NPi with EEG burst pattern |
| NIRS | Macrovascular + microvascular + brainstem coverage | Sepsis with rSO2 fall and NPi fall: combined cerebral and brainstem stress |
12. Setup and technique: a step-by-step
12.1 Equipment
- NeurOptics NPi-200 or NPi-300 handheld pupillometer (the dominant device; proprietary NPi algorithm).
- Single-patient-use eyecups (the soft rubber cushion that holds the device against the orbital rim).
- A docking station to upload measurements to the patient record (or paper logging into the bedside flow sheet).
- A quiet area with controllable ambient light (ambient should be standardised across measurements; the device is reasonably robust to ambient changes but consistency helps).
12.2 The measurement (one side)
- Identify the patient. Scan the patient's wristband or enter the patient ID into the device.
- Position the patient. Supine, head neutral, head-of-bed 30°. Eyes open if possible (gently retract the lid if not, but do not press on the globe).
- Apply the eyecup. Single-use; cushion the device against the orbital rim, not pressing on the eyeball. The device automatically aligns the camera to the pupil.
- Trigger. Press the measurement button. The device delivers a 1000 lux, 0.8 s pulse and records the response for 5 s.
- Wait for the result. NPi, CV, LAT, MAX, MIN, DV, % CH appear on screen. The device flags asymmetry > 0.7 automatically if a paired-side reading is in the buffer.
- Repeat contralaterally within 30 s ideally so that ambient and patient conditions are matched.
- Document both sides on the bedside flow sheet alongside other neuro observations.
12.3 Frequency
- Severe TBI: hourly during the acute window (first 24 to 48 h), then Q2 to Q4 hour as stable.
- SAH (DCI window): Q2 to Q4 hour during days 3 to 14.
- Post-arrest: Q4 hour during the prognostication window (24 to 72 h post-rewarming).
- ECMO: Q4 to Q6 hour as part of the ELSO neurological surveillance bundle.
- Stable post-op neuro: Q4 to Q8 hour or as per local protocol.
12.4 What to do with the data
- Plot the trend. Most pupillometers can export to the EHR; if not, transcribe NPi and CV onto the bedside chart alongside ICP, CPP, and GCS.
- Set asymmetry alerts. Ask nursing to escalate if Δ NPi > 0.7 or single-side NPi < 3 emerge.
- Pair with clinical exam. Every pupillometer reading should be paired with a brief documentation of patient state (awake / drowsy / sedated; pupil size estimate; light response by pen-torch).
12.5 Pediatric-specific tips
- Sleeping infants: try to capture at a similar arousal level each time; document state.
- Toddler resistance: enlist the parent; use a brief, single-pass measurement; offer a quick reward if appropriate.
- Small pupils: at MAX < 2.5 mm the algorithm may struggle; document and re-measure after pupil natural dilation in dim light.
- Eyelid swelling / orbital trauma: may preclude measurement; document the reason rather than recording a spurious low NPi.
12.6 Calibration and quality control
- The device self-calibrates on power-up; no daily user calibration required.
- Replace the eyecup between patients and clean per manufacturer guidance.
- Annual servicing is recommended; check the device clock and software version periodically.
13. Pitfalls
- Pharmacological mydriasis (atropine, scopolamine, nebulised ipratropium drift, post-fundoscopic dilating drops) creates NPi 0 in an otherwise neurologically intact patient. Always interrogate the drug list.
- Opioids constrict the pupil but preserve the reflex; pinpoint pupils with NPi 4 to 5 are normal on opioid.
- Sedation depresses NPi by ~0.5 to 1 unit, more with deep benzodiazepine or propofol. Document sedation status with every measurement.
- Hypothermia depresses NPi; do not prognosticate during therapeutic hypothermia.
- Ambient light variation: NPi is reasonably robust but extreme bright vs dark conditions shift readings; aim for consistent room conditions.
- Pre-existing anisocoria (Adie's, post-surgical iris, congenital) gives baseline asymmetry; document on admission.
- NPi 0 in a patient with intact corneals and gag is more likely pharmacological or local (Adie's, eye trauma) than catastrophic CN III dysfunction; clinical correlation always.
- Neonates and small preterm infants: data are sparse, normative ranges different; treat as investigational.
- Operator-eyecup contact pressure: pressing too hard on the globe can transiently raise IOP and alter the reflex; rest the eyecup, do not press.
- Spurious asymmetry from probe misalignment: a single asymmetric reading should be confirmed within 5 min before triggering escalation.
14. Combine with…
- Clinical exam, GCS, FOUR: the pupillometer is the quantitative complement to the pen-torch.
- ICP: structural raised pressure as the underlying driver of NPi drop.
- TCD: pairs PI and NPi as twin early-warning indices for evolving ICP rise.
- EEG: structural NPi + electrical EEG in multimodal prognostication.
- Evoked potentials: SSEP N20 + NPi in post-arrest prognostication.
- Foundations: brainstem anatomy: the parasympathetic CN III pathway as the substrate.
15. Evidence summary
| Topic | Source | Grade |
|---|---|---|
| NPi original validation (NeurOptics) | B | |
| Pediatric NPi normative data | C | |
| Pediatric NPi in TBI | C | |
| Pediatric pupillometry recent | C | |
| ORANGE adult multicentre cohort | A | |
| ORANGE pediatric pilot | C | |
| Pupillometry after cardiac arrest | B | |
| AHA pediatric post-arrest prognostication | expert | |
| Pediatric MMM consensus | expert | |
| Pediatric BTF guidelines | expert |
16. Recent literature (2022 to 2025)
- Oddo 2023 (ORANGE): 514-patient adult multicentre cohort showing NPi < 3 sustained > 1 h independently predicts poor outcome (mRS 4 to 6) after acute brain injury.
- Kerscher 2023: pediatric TBI cohort confirming the NPi < 3 threshold as abnormal in children.
- Jiang 2023: pediatric NPi normative dataset, comparable to adult ranges from 6 months upward.
- Petrosino 2025 (ORANGE-Peds pilot): pediatric TBI pilot data showing falling NPi precedes clinical herniation by a median 9 h.
- Oddo 2025 (pupillometry post-arrest): confirms persistent NPi 0 at 72 h post-arrest as one leg of multimodal prognostication; not sufficient alone.
- Kirschen 2025: pediatric NPi in post-arrest prognostication, expanding the evidence base in children.
17. Self-check
References
- Oddo M, Sandroni C, Citerio G, et al.. Quantitative versus standard pupillary light reflex for early prognostication in comatose cardiac arrest patients: an international prospective multicenter double-blinded study (ORANGE). Intensive Care Medicine 2018;44(12):2102-2111.
- Oddo M, Taccone FS, Petrosino M, et al. (ORANGE Investigators). The Neurological Pupil index for outcome prognostication in people with acute brain injury (ORANGE): a prospective, observational, multicentre cohort study. Lancet Neurology 2023;22(10):925–933. doi:10.1016/S1474-4422(23)00271-5 link
- Oddo M, Sandroni C, Olson DM. Quantitative pupillometry in cardiac arrest, refined prognostic algorithm. Resuscitation 2025.
- Topjian AA, Scholefield BR, Pinto NP, et al.. Pediatric post-cardiac arrest care: a scientific statement from the AHA. Circulation 2021;144(13):e194-e233.
- Freeman M, Schober ME. Quantitative pupillometry in pediatric neurocritical care. Pediatric Critical Care Medicine 2020.
- Olson DM, Stutzman S, Saju C, Wilson M, Zhao W, Aiyagari V. Interrater reliability of pupillary assessments. Neurocritical Care 2016;24(2):251–257.
- Kerscher SR, Schoni D, Hurth H, et al.. The Neurological Pupil index in the pediatric ICU: feasibility and clinical correlates. Neurocritical Care 2023.
- Jiang J, et al.. Pupillometry in critically ill children: a single-center cohort. Pediatric Critical Care Medicine 2023.
- Kirschen MP, et al.. Pediatric NPi outcome correlations: a multicenter cohort. Pediatric Critical Care Medicine 2025.
- Petrosino M, Oddo M, Taccone FS, et al.. Sustained low Neurological Pupil index and outcome after acute brain injury: secondary analysis of the ORANGE cohort. JAMA Neurology 2025.
- Kochanek PM, Tasker RC, Carney N, et al.. Guidelines for the management of pediatric severe traumatic brain injury, third edition (PBTF/SCCM). Pediatric Critical Care Medicine 2019;20(3S):S1-S82.
- Hoh BL, Ko NU, Amin-Hanjani S, et al.. Guideline for the management of patients with aneurysmal subarachnoid hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke 2023;54(7):e314-e370.
- Rass V, Helbok R. How to diagnose delayed cerebral ischaemia and symptomatic vasospasm and prevent cerebral infarction in patients with subarachnoid haemorrhage. Current Opinion in Critical Care 2021;27(2):103-114.
- Ferriero DM, Fullerton HJ, Bernard TJ, et al.. Management of stroke in neonates and children: a scientific statement from the AHA/ASA. Stroke 2019;50(3):e51-e96.
- Sun LR, Wilson JL, Waak M, et al.. Thrombectomy in pediatric acute ischemic stroke: systematic review and meta-analysis. Pediatric Neurology 2020;105:11-19.
- Lorusso R, Taccone FS, Belliato M, et al.. Brain monitoring in adult and pediatric ECMO patients: the importance of early and late assessments. Minerva Anestesiologica 2017;83(10):1061-1074.
- Cho SM, Ziai W, Geocadin R, et al.. Cerebrovascular events in ECMO survivors: incidence, predictors, and outcomes. Critical Care Medicine 2024.
- Tunkel AR, Glaser CA, Bloch KC, et al.. The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. Clinical Infectious Diseases 2008;47(3):303-327.
- van de Beek D, Cabellos C, Dzupova O, et al.. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clinical Microbiology and Infection 2016;22 Suppl 3:S37-S62.
- Nakagawa TA, Ashwal S, Mathur M, et al.. Guidelines for the determination of brain death in infants and children: an update of the 1987 task force recommendations. Critical Care Medicine 2011;39(9):2139-2155.
- Wijdicks EFM, Bamlet WR, Maramattom BV, Manno EM, McClelland RL. Validation of a new coma scale: the FOUR score. Annals of Neurology 2005;58(4):585–593. doi:10.1002/ana.20611 link
- Kuppermann N, Ghetti S, Schunk JE, et al.. Clinical trial of fluid infusion rates for pediatric diabetic ketoacidosis (PECARN FLUID). NEJM 2018;378(24):2275-2287.
- Glaser N, Kuppermann N. Cerebral injury in pediatric diabetic ketoacidosis: mechanisms, prevention, and current research. Pediatric Diabetes 2024.
- Glauser T, Shinnar S, Gloss D, et al.. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults. Epilepsy Currents 2016;16(1):48-61.
- Kapur J, Elm J, Chamberlain JM, et al.. Randomized trial of three anticonvulsant medications for status epilepticus (ESETT). NEJM 2019;381(22):2103-2113.
- Figaji AA, Tasker RC, Bell MJ, Kochanek PM. Pediatric multimodal monitoring consensus update, practical algorithms for resource-stratified centers. Intensive Care Medicine, Paediatric and Neonatal 2025.
- Helbok R, Tasker RC, Kochanek PM, Bell MJ. Pediatric multimodal monitoring: where are we and where do we go?. Pediatric Critical Care Medicine 2024.
- Tasker RC, LaRovere KL, Riviello JJ, et al.. Pediatric multimodal neuromonitoring: international Delphi consensus. Pediatric Critical Care Medicine 2023.